

Search
Statistics
We have 222 registered usersThe newest registered user is raheelmemon
Our users have posted a total of 1140 messages in 613 subjects
If you are seeing this, you have attempted to link to the UpToDate widget but are experiencing a problem. Please visit UpToDate for more information.

An Algorithm-Based Approach to First-Episode Schizophrenia
3 posters
FORUM FOR PSYCHIATRY RESIDENTS :: Psychiatry :: Psychiatry-Neurology-Psychology discussion :: Psychiatry In Depth
Page 1 of 1

An Algorithm-Based Approach to First-Episode Schizophrenia
![]() Admin Sun Dec 09, 2012 8:04 pm
Admin Sun Dec 09, 2012 8:04 pm
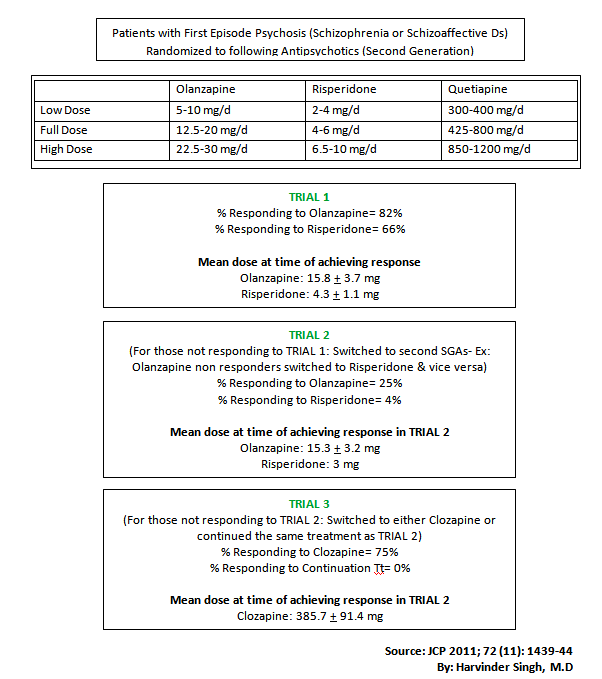
An Algorithm-Based Approach to First-Episode Schizophrenia
J Clin Psychiatry 72(11):1439-44 (2011)
J Clin Psychiatry 72(11):1439-44 (2011)
Note the difference of response between first & second trials and inclusion of Clozapine trial after 2 trails.
Also most focus of this approach is on Risperidone, Olanzapine & Clozapine.
The findings of Olanzapine > Risperidone is in line with CATIE trial.
Questions for all forum members:
- Is Clozapine not superior when used as first line?
- Is First Generation Antipsychotics < Second generations as first line?
- What is your personal experience and choice of antipsychotics for pt with first episode schizophrenia

Admin- Admin

- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -

Re: An Algorithm-Based Approach to First-Episode Schizophrenia
![]() adisuper Tue Dec 11, 2012 8:18 am
adisuper Tue Dec 11, 2012 8:18 am
what i m observing during my residency is that these patients with 1st episode of schizophrenia and those with ATPD responds best to haloperidol(we generaly give 5mg TDS).
in some young patients with a short history there is a dramatic improvement in 2-3 days.
There is no evidence for differences in efficacy between atypical and typical antipsychotics, but there was a clear difference in the side-effect profile.
source:Efficacy of atypical v. typical antipsychotics in the treatment of early psychosis: meta-analysis Nicolas A. Crossley, MRCPsych, MSc and Miguel Constante, MRCPsych; Philip McGuire, FRCPsych, PhD; Paddy Power, MRCPsych, FRANZCP, MD, The British Journal of Psychiatry (2010)196: 434-439
in some young patients with a short history there is a dramatic improvement in 2-3 days.
There is no evidence for differences in efficacy between atypical and typical antipsychotics, but there was a clear difference in the side-effect profile.
source:Efficacy of atypical v. typical antipsychotics in the treatment of early psychosis: meta-analysis Nicolas A. Crossley, MRCPsych, MSc and Miguel Constante, MRCPsych; Philip McGuire, FRCPsych, PhD; Paddy Power, MRCPsych, FRANZCP, MD, The British Journal of Psychiatry (2010)196: 434-439
adisuper- Posts : 28
Points : 32
Reputation : 0
Join date : 2012-06-04
Re: An Algorithm-Based Approach to First-Episode Schizophrenia
![]() Admin Wed Dec 12, 2012 10:50 pm
Admin Wed Dec 12, 2012 10:50 pm
Thanks for sharing your experience Adisuper.
We also prefer Haloperidol & Risperidone in most first episode psychosis.
After reading that Algorithm approach article, I would prefer SGA over FGA (side effect profile issue). Good reference while explaining to high functioning patients and for those with curious family members.
Isn't 5mg TDS a large dose. Is that because of non response to lower doses? Just curious.
Thanks again.

Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: An Algorithm-Based Approach to First-Episode Schizophrenia
![]() adisuper Sat Dec 15, 2012 10:32 am
adisuper Sat Dec 15, 2012 10:32 am
yes 5mg TDS is indeed a large dose but here we generaly start with it in young pts. with no medical co-morbidity as at this dose response is quick and if EPS do occurs(it occurs in 2 in 10 pts on this dose) we add anticholinergics. We use this approach as village patients want a quick response and r otherwise inclined to faith healers.
no documented evidence of using such dose its just experience of my prof.
no documented evidence of using such dose its just experience of my prof.
adisuper- Posts : 28
Points : 32
Reputation : 0
Join date : 2012-06-04

Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: An Algorithm-Based Approach to First-Episode Schizophrenia
![]() P450 Thu Dec 20, 2012 12:15 am
P450 Thu Dec 20, 2012 12:15 am
One large study, EUFEST, should help guide us in the treatment for first-episode schizophrenia:
Summary
Background Second-generation antipsychotic drugs were introduced over a decade ago for the treatment of schizophrenia; however, their purported clinical eff ectiveness compared with first-generation antipsychotic drugs is still debated. We aimed to compare the effectiveness of second-generation antipsychotic drugs with that of a low dose of haloperidol, in first-episode schizophrenia. Methods We did an open randomised controlled trial of haloperidol versus second-generation antipsychotic drugs in 50 sites, in 14 countries. Eligible patients were aged 18–40 years, and met diagnostic criteria for schizophrenia,
schizophreniform disorder, or schizoaffective disorder. 498 patients were randomly assigned by a web-based online system to haloperidol (1–4 mg per day; n=103), amisulpride (200–800 mg per day; n=104), olanzapine (5–20 mg per day; n=105), quetiapine (200–750 mg per day; n=104), or ziprasidone (40–160 mg per day; n=82); follow-up was at 1 year. The primary outcome measure was all-cause treatment discontinuation. Patients and their treating physicians were not blinded to the assigned treatment. Analysis was by intention to treat. This study is registered as an International Standard Randomised Controlled Trial, number ISRCTN68736636.
Findings
The number of patients who discontinued treatment for any cause within 12 months was 63 (Kaplan-Meier estimate 72%) for haloperidol, 32 (40%) for amisulpride, 30 (33%) for olanzapine, 51 (53%) for quetiapine, and 31 (45%) for ziprasidone. Comparisons with haloperidol showed lower risks for any-cause discontinuation with amisulpride (hazard ratio
0·37, [95% CI 0·24–0·57]), olanzapine (HR 0·28 [0·18–0·43]), quetiapine (HR 0·52
[0·35–0·76]), and ziprasidone (HR 0·51 [0·32–0·81]). However, symptom reductions were virtually the same in all the groups, at around 60%.
Interpretation
This pragmatic trial suggests that clinically meaningful antipsychotic treatment of first-episode of schizophrenia is achievable, for at least 1 year. However, we cannot conclude that second-generation drugs are more efficacious than is haloperidol, since discontinuation rates are not necessarily consistent with symptomatic improvement.
Regarding haldol dosing as per EUFEST data:
"The maximum dose of haloperidol was set at 4 mg per day, since studies have suggested that patients with first-episode schizophrenia respond to low doses of antipsychotic drugs.19,20 Furthermore, higher doses do not increase the antipsychotic effect of haloperidol, but do increase the risk of side-effects, especially in patients with first-episode schizophrenia.21–26"
Effectiveness of antipsychotic drugs in first-episode
schizophrenia and schizophreniform disorder: an open
randomised clinical trial. Lancet 2008; 371: 1085–97.
Summary
Background Second-generation antipsychotic drugs were introduced over a decade ago for the treatment of schizophrenia; however, their purported clinical eff ectiveness compared with first-generation antipsychotic drugs is still debated. We aimed to compare the effectiveness of second-generation antipsychotic drugs with that of a low dose of haloperidol, in first-episode schizophrenia. Methods We did an open randomised controlled trial of haloperidol versus second-generation antipsychotic drugs in 50 sites, in 14 countries. Eligible patients were aged 18–40 years, and met diagnostic criteria for schizophrenia,
schizophreniform disorder, or schizoaffective disorder. 498 patients were randomly assigned by a web-based online system to haloperidol (1–4 mg per day; n=103), amisulpride (200–800 mg per day; n=104), olanzapine (5–20 mg per day; n=105), quetiapine (200–750 mg per day; n=104), or ziprasidone (40–160 mg per day; n=82); follow-up was at 1 year. The primary outcome measure was all-cause treatment discontinuation. Patients and their treating physicians were not blinded to the assigned treatment. Analysis was by intention to treat. This study is registered as an International Standard Randomised Controlled Trial, number ISRCTN68736636.
Findings
The number of patients who discontinued treatment for any cause within 12 months was 63 (Kaplan-Meier estimate 72%) for haloperidol, 32 (40%) for amisulpride, 30 (33%) for olanzapine, 51 (53%) for quetiapine, and 31 (45%) for ziprasidone. Comparisons with haloperidol showed lower risks for any-cause discontinuation with amisulpride (hazard ratio
0·37, [95% CI 0·24–0·57]), olanzapine (HR 0·28 [0·18–0·43]), quetiapine (HR 0·52
[0·35–0·76]), and ziprasidone (HR 0·51 [0·32–0·81]). However, symptom reductions were virtually the same in all the groups, at around 60%.
Interpretation
This pragmatic trial suggests that clinically meaningful antipsychotic treatment of first-episode of schizophrenia is achievable, for at least 1 year. However, we cannot conclude that second-generation drugs are more efficacious than is haloperidol, since discontinuation rates are not necessarily consistent with symptomatic improvement.
Regarding haldol dosing as per EUFEST data:
"The maximum dose of haloperidol was set at 4 mg per day, since studies have suggested that patients with first-episode schizophrenia respond to low doses of antipsychotic drugs.19,20 Furthermore, higher doses do not increase the antipsychotic effect of haloperidol, but do increase the risk of side-effects, especially in patients with first-episode schizophrenia.21–26"
Effectiveness of antipsychotic drugs in first-episode
schizophrenia and schizophreniform disorder: an open
randomised clinical trial. Lancet 2008; 371: 1085–97.
P450- Moderator

- Posts : 34
Points : 34
Reputation : 0
Join date : 2012-01-15
» Schizophrenia Discussion Thread.
» Schizophrenia & Functional Capacity
» Suicide Risk in First Episode Psychosis
» APA Course: Buprenorphine and Office-Based Treatment of Opioid Dependence
» Evidence-Based Guideline: Treatment of Tardive Syndromes
» Schizophrenia & Functional Capacity
» Suicide Risk in First Episode Psychosis
» APA Course: Buprenorphine and Office-Based Treatment of Opioid Dependence
» Evidence-Based Guideline: Treatment of Tardive Syndromes
FORUM FOR PSYCHIATRY RESIDENTS :: Psychiatry :: Psychiatry-Neurology-Psychology discussion :: Psychiatry In Depth
Page 1 of 1
Permissions in this forum:
You cannot reply to topics in this forum
» L-Methylfolate: Who Will benefit
» Vitamins & Supplements in Clinical Practice.
» Imaging Biomarkers for Outcomes in Mild TBI
» Q.5 Clozapine Neutopenia
» Treating Disorders!
» Cortical Abnormalities in Adults & Adolescents with MDD
» Efficacy of Antipsychotics in Pediatric Acute Mania
» Obsessive Compulsive Disorder in Adults: Which Treatment is Better?