

The newest registered user is raheelmemon
Our users have posted a total of 1140 messages in 613 subjects

ABPN Initial Certification Exam 2015
FORUM FOR PSYCHIATRY RESIDENTS :: Psychiatry :: Psychiatry-Neurology-Psychology discussion :: Psychiatry In Depth
Page 1 of 3 • 1, 2, 3 ![]()

ABPN Initial Certification Exam 2015
![]() Admin Sat Aug 29, 2015 8:28 pm
Admin Sat Aug 29, 2015 8:28 pm

This thread is dedicated to ABPN (American Board of Psychiatry and Neurology) Initial Certification Exam 2015.
Exam Date: September 24-25, 2015
High yield topics will be posted here frequently over the course of next 1 month.
Index
Page 1:
1. Adjunctive use of Antidepressants for Bipolar Disorder (per recent ISBD Guidelines).
2. Lithium Facts (Not indicated in; Contraindications; Medications increasing/decreasing level; association with kidney function & thyroid).
3. Medications associated with symptoms of restless legs syndrome.
4. REM Sleep Changes in Depression.
5. Antipsychotics least likely to exacerbate OCD symptoms in patients with comorbid OCD and schizophrenia.
6. Neurochemical Abnormalities in Catatonia.
7. Neuropsychiatric Complications of Glucocorticoid Use.
8. Antipsychotics Effect on Prolactin levels in patients with breast cancer.
9. What is the Difference Between Amphetamine and Methylphenidate?
10. ECT and Contraindications.
11. Brain structures involved in Anxiety.
12. New Recommendations for Hydroxyzine (European Medicines Agency).
13. Major depressive disorder vs bereavement.
14. Identifying Dementia patient at risk of unsafe Driving.
Page 2:
15. Alzheimer's disease: Early onset vs Late onset.
16. Medications for Alcohol Dependence + Naltrexone Mechanism.
17. Aphasia types.
18. Antidepressant in Treating or Preventing Depression Emerging During HCV (Hepatitis C) Treatment.
19. Narcolepsy with Cataplexy: Treatment
20. Bipolar I vs ADHD in Children + Treatment of ADHD and Comorbid Bipolar Disorder.
21. Factitious Disorders Management Recommendations.
22. Treatment of Persistent Aggressive Behaviors in Schizophrenia.
23. Bipolar disorder type II vs Borderline Personality Disorder.
24. Management of Behavioral and Psychological Symptoms of Dementia.
25. Donepezil, Rivastigmine & Galantamine: Use in Renal and Hepatic Impairment.
26. Mechanism of action of medications approved for weight loss.
27. Flibanserin Contraindications.
28. Antipsychotic Drug Use and the Risk of Seizures.
29. Rates of Placental Passage of Antipsychotics.
Page 3:
30. Treatment Options of Sexually Inappropriate Behavior in Dementia.
31. Acute Stress Disorder and Psychological debriefing.
32. Sleep Changes in Children and Elderly.
33. Personality Disorder and Defense Mechanisms
34. Neuro-Oncology: Important Histopathology Findings.
35. Basal Ganglia Structures and Diseases Associated with Damage.
36. Hippocampal Formation changes in Schizophrenia.
37. Antipsychotics least likely to increase QTc interval.
38. Model of Opioid Dysfunction and Buprenorphine Treatment in Borderline Personality Disorder.
39. Juvenile Myoclonic Epilepsy.
40. Poor & Good Prognostic Factors in Conversion Disorder.
41. Important EEG Findings.
42. Intellectual Disability Common Causes.
43. Anorexia Nervosa & Metabolic Abnormalities.
44. Pedophilic Disorder: Good and Bad Prognosis Indicators
Page 4:
45. Psychodynamic themes in Panic Disorder.
46. Sleep Stages & EEG Findings.
47. Postulated brain regions involved in different symptoms of ADHD.
48. Foods Avoided with MAOIs.
49. fMRI and Postmortem biopsy findings in Depression.
50. Antidepressants & False Positive Screen for Amphetamine.
51. FDA Approved Medications for Sleep Disorders.
52. Visual developmental milestones.
53. Children developmental milestones (important).
54. Psychopharmacology: Important CYP450 Interactions (*)
55. Incidence Rate and Period Prevalence.
56. Biostatistics.
57. Visual Pathway And Associated Visual Defects.
57. Peripheral Nerves: Radial, Ulnar, Median and Musculocutaenous.
58. Drug of Choice for Psychosis in Parkinson's Disease.
Page 5:
60. Erikson's stages of psychosocial development.

Last edited by Admin on Sat Sep 19, 2015 8:07 pm; edited 54 times in total

Admin- Admin

- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -

Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Aug 29, 2015 8:35 pm
Admin Sat Aug 29, 2015 8:35 pm
According to International Society for Bipolar Disorders (ISBD) Recent Recommendations: Adjunctive use of Antidepressants for Bipolar Disorder is Considered in following conditions:
(a) In bipolar I and II in acute depressive episodes when there is a history of a positive response to antidepressants.
(b) In maintenance treatment when a patient relapses into a depression after the antidepressant is discontinued.
Last edited by Admin on Sun Aug 30, 2015 4:35 pm; edited 1 time in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Aug 29, 2015 8:58 pm
Admin Sat Aug 29, 2015 8:58 pm

* less effective in bipolar disorder with mixed features and rapid cycling.
* Lithium directly inhibits Glycogen Synthase Kinase 3B & Inositol monophosphate Phosphatase
* Contraindications for Lithium use—
- Significant renal impairment
- Sodium depletion
- Dehydration
- Significant cardiovascular disease (lithium can rarely cause sinus node dysfunction- eg, sinus bradycardia and sinoatrial block; atrioventricular node dissociation with atrioventricular block and junctional rhythms; and ventricular premature beats).
- Psoriasis, which lithium exacerbates, is a relative contraindication.
* Levels ≥ 2.5 mEq/L (2.5 mmol/L) constitute a medical emergency, even in patients who appear relatively asymptomatic.
* Medications that Increases lithium level
> Thiazide diuretics
> Nonsteroidal antiinflammatory drugs (NSAIDS) except aspirin
> Angiotensin converting enzyme (ACE) inhibitors
> Antibiotics tetracyclines and metronidazole
* Medications that Decreases lithium level
> Potassium-sparing diuretics
> Theophylline
* Clinicians should consult a nephrologist and discontinue lithium when the serum creatinine approaches or exceeds 1.6 mg/dL (140 mmol/L). The most important risk factor for renal damage from lithium is repeated episodes of lithium intoxication.
* Neither pretreatment hypothyroidism (presumably treated adequately with T4) nor lithium-induced hypothyroidism is a contraindication to lithium therapy. Reasonable recommendations are to monitor serum TSH and if it rises much above the upper value of normal, to start T4 while continuing the lithium.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sun Aug 30, 2015 4:35 pm
Admin Sun Aug 30, 2015 4:35 pm
Drugs that can be associated with symptoms of restless legs syndrome:
- Alcohol
- Nicotine
- Caffeine
- Serotonergic antidepressants
- Antipsychotics
- Dopamine-blocking antiemetics (eg, metoclopramide)
- Centrally-acting antihistamines
In a study of over 1600 patients, primarily males, the antidepressants with the highest likelihood of exacerbating RLS symptoms were citalopram, paroxetine, fluoxetine, and amitriptyline.
In another study, mirtazapine appeared to have the highest risk of RLS among second-generation antidepressants
Among the above choices, Wellbutrin is best option for least/no serotonoergic activity.
Source: www.rls.org/Document.Doc?id
J Clin Sleep Med. 2010 Feb;6(1):79-83.
J Psychiatr Res. 2008 Nov;43(1):70-5. Epub 2008 May 12.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sun Aug 30, 2015 4:40 pm
Admin Sun Aug 30, 2015 4:40 pm
REM Sleep Changes in Depression:
- Decreased REM latency
- Increased number of REM
- Increased amount of REM
- Shift in REM distribution to most occurring in first half of night

Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sun Aug 30, 2015 4:46 pm
Admin Sun Aug 30, 2015 4:46 pm
Antipsychotics least likely to exacerbate OCD symptoms in patients with comorbid obsessive–compulsive disorder (OCD) and schizophrenia ("Schizo-Obsessive"):
Atypical antipsychotics (Dopamine-Serotonin Antagonist) are more likely to exacerbate Obsessive Compulsive symptoms (OCS), compared to typical antipsychotics.
Mechanism: Atypical antipsychotics (Dopamine-Serotonin Antagonist) blocks 5HT2A receptor in presynaptic dopamine neuron --> disinhibit dopaminergic activity --> postulated to increase OCS in pt with schizophrenia.
Amisulpride: new atypical antipsychotic is selective dopamine blocker, with low affinity for 5HT2A receptor --> resultant antiobsessional effects.
Source: Kim SW et al. J Clin Psychopharmacol. 2008;28:349-352.
Second option after Amisulpride is Aripiprazole. Aripiprazole is potent 5HT2A antagonist with Partial dopamine agonist --> thus causing relatively weak dopamine D2 blockade --> thus pharmacologically even Aripiprazole can result in excacerbation of OCS symptoms. However following two studies (small open label prospective study and double blind trial) showed efficacy of Aripiprazole in OCS in schizophrenia.
Source: Sayyah M. Depress Anxiety. 2012;29:850-854., Kim SW, Clinc Neuropsychopharmacol 2009;32:243-249.
Also read Psychiatric Annals Oct 2013 issue on Comorbidities in Schizophrenia.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sun Aug 30, 2015 4:49 pm
Admin Sun Aug 30, 2015 4:49 pm
Neurochemical Abnormalities in Catatonia:
- Low GABA activity in the frontal cortex
- Low dopamine (D2) activity in the basal ganglia
- High glutamate—N-methyl-D-aspartate (NMDA)—activity in the parietal cortex
- or combination of these
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sun Aug 30, 2015 4:51 pm
Admin Sun Aug 30, 2015 4:51 pm
DOSE EQUIVALENCY:
Hydrocortisone (cortisol) 25mg= Prednisone 5mg= Methylprednisolone 4 mg= Dexamethasone 0.5 mg= Betamethasone 0.6 mg
AFFECTIVE, BEHAVIORAL, AND COGNITIVE CHANGES ASSOCIATED WITH STEROIDS
Rome and Braceland (1952) defined four grades of psychiatric responses in 20 patients receiving cortisone and ACTH:
* Grade 1: general feeling of well-being and stimulation, with improved concentration, energy, and clarity of thought.
* Grade 2: more distinct elevation of mood accompanied by restlessness, insomnia, increased motor activity, and accelerated mental activity.
* Grade 3: severe anxiety, ruminations, obsessions, mood swings, lethargy, indifference, crying spells, hopelessness and helplessness, excitement, restlessness, and flight of ideas.
* Grade 4: hallucinations, delusions, and “extreme variations in mood”.
Note: 60% fell into grades 1 and 2.
(Source: Am J Psychiatry 1952; 108:641– 651)
Lewis and Smith (1983) conducted a retrospective study of 14 cases and 79 published case reports of steroid induced psychiatric syndromes; and found:-
depression (35%), mania (31%), psychosis (14%), delirium (13%), and mixed states (6%).
(Source: J Affect Disord 1983; 5:319 –332)
The most common cognitive deficit: verbal or declarative memory.
DOSE–RESPONSE RELATIONSHIP
According to Boston Collaborative Drug Surveillance Program (studied 718 consecutive hospitalized patients receiving prednisone therapy in 1972):
Incidence of psychiatric symptoms in patients on:
40 mg/day: 1.3%
41–80 mg/day: 4.6%
>80 mg/day: 18.4%.
(Source: Clin Pharmacol Ther Sep–Oct 1972; 13(5):694 –698)
Also Lewis and Smith (1983) found that 77% of patients developed psychiatric symptoms when prednisone doses of >40mg is used.
TIME COURSE FOR DEVELOPMENT OF NEUROPSYCHIATRIC EFFECTS
According to Lewis and Smith (1983) patients developed symptoms:
- within first 6 weeks: 89%
- within the first 2 weeks: 62%
- within the first week: 39%
They found a median of 11.5 days (hours- 210 days) from initiation of steroid to development of neuropsychiatric manifestations.
>90% patients recovered from steroid related neuropsychiatric manifestations within 6 weeks.
CLINICAL PREDICTORS FOR NEUROPSYCHIATRIC EFFECTS
(A) STEROID DOSE:
- as discussed above
(B) GENDER:
- Female gender at risk.
- Lewis and Smith (1983) found that 68% of patients with psychiatric effects were women.
- This predominance persisted even when cases of SLE and rheumatoid arthritis were excluded.
(C) AGE:
- Age has been not reported as risk factor.
- Lewis and Smith (1983) found mean age to be 39.6 years (range 8–71 years).
(D) LIVER OR RENAL DYSFUNCTION:
Patient with liver or renal dysfunction (as well as the elderly) have higher free levels (unbound by albumin or transcortin) of prednisolone, so may be at higher risk for side effects.
(E) BLOOD BRAIN DAMAGE & LOW SERUM COMPLEMENT:
Nishimura and associates conducted a prospective cohort study of risk factors for corticosteroidinduced psychiatric disorders in patients with SLE. They identified blood brain barrier damage (odds ratio [OR] 33.3) and low serum complement levels (OR 0.91) as independent risk factors for steroid-induced neuropsychiatric disturbances.
(Source: Psychoneuroendocrinology 2008; 33(3):395–403)
1. Discontinue steroids, OR
2. Decrease dose <40 mg/day of prednisone equivalent.
3. No FDA Approved medication available.
ANTIDEPRESSANTS:
- Most studies warn against the use of TCAs: because of anticholinergic effects exacerbating delirium and worsening of symptoms could occur.
- Case reports of success with SSRI and SNRI, but no clinical trial done.
MOOD STABILIZERS:
- Reports of success with Lithium, Valproate and Lamotrigine.
- Clinical trial done by Falk et al compared 27 patients (given lithium before corticosteroids) with 44 controls (receiving only corticosteroids).
No patients in the lithium treated group developed psychiatric symptoms, and 6/44 (14%) of the controls developed psychosis.
Source: JAMA 1979; 241:1011–1012
ANTIPSYCHOTICS:
- Low dose antipsychotics are effective.
- Davis et al found that low-dose neuroleptic treatment led to resolution of psychotic symptoms in 83% of patients (24/29):-
*33% responded in 3 days
*60% improved in 1 week
* 80% have resolution of symptoms in 2 weeks.
Source: Psychiatr Ann 1992; 22:487–491
(For details please refer to: Psychosomatics 2012:53:103–115)

Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sun Aug 30, 2015 4:58 pm
Admin Sun Aug 30, 2015 4:58 pm
Antipsychotics Effect on Prolactin levels in patients with breast cancer
Antipsychotics that increases prolactin (45 to >100 ng/ml) and should be AVOIDED in patients with breast cancer:
Risperidone
Paliperidone
Haloperidol
Antipsychotics that increases prolactin (20-50 ng/ml) and should be CAUTIONED in patients with breast cancer:
Olanzapine
Iloperidone
Lurasidone
Antipsychotics that increases minimal prolactin and are PREFERRED in patients with breast cancer:
Ziprasidone
Asenapine
Quetiapine
Clozapine
Antipsychotic that may lower prolactin and is PREFERRED in patients with breast cancer:
Aripiprazole
Source: Am J Psychiatry 2014;171:616-621.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sun Aug 30, 2015 5:02 pm
Admin Sun Aug 30, 2015 5:02 pm
What is the Difference Between Amphetamine and Methylphenidate?
(1) Both increase synaptic DA (Dopamine) and NE (Norepinephrine) levels, but only amphetamine enhances release as well as blocks reuptake of NE and DA (especially at high doses).
(2) Unlike methylphenidate, amphetamine is a competitive inhibitor at Dopamine Transporter, thus competing with DA. By this mechanism amphetamine itself is transported into the DA terminal.
(3) Amphetamine is also a competitive inhibitor of vesicular monoamine transporter (a property that methylphenidate lacks).
Source: Stahl's Illustrated Attention Deficit Hyperactivity Disorder
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sun Aug 30, 2015 5:06 pm
Admin Sun Aug 30, 2015 5:06 pm
ECT and Contraindications:
(1) There are no "absolute" medical contraindications to ECT.
(2) Situations exist in which ECT is associated with an increased likelihood of serious morbidity or mortality. For such patients, the decision to administer ECT should be based upon the premise that their psychiatric condition is grave and that ECT is the safest treatment available.
3) Careful medical evaluation of risk factors should be carried out prior to ECT, with specific attention to modifications of the patient's management and the administration of ECT which may diminish the level of risk.
4) Specific conditions that may be associated with substantially increased risk include the following:
a) unstable or severe cardiovascular conditions such as recent myocardial infarction, poorly compensated congestive heart failure, and severe valvular cardiac disease.
b) aneurysm or vascular malformation that might be susceptible to rupture with increased blood pressure.
c) increased intracranial pressure, as may occur with some brain tumors or other space-occupying cerebral lesions.
d) recent cerebral infarction.
e) pulmonary conditions such as severe chronic obstructive pulmonary disease, asthma, or pneumonia.
f) anesthetic risk rated as ASA level 4 or 5.
Source: http://www.ect.org/resources/apa/3.html
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Tue Sep 01, 2015 8:04 pm
Admin Tue Sep 01, 2015 8:04 pm
Brain structures involved in Anxiety:
* Brain Stem: Locus ceruleus (Nor Epinephrine) and Raphe Nucleus (Serotonin)
* Amygdala (Anticipatory anxiety)
* Prefrontal Cortex (Phobic avoidance)
* Cingulate Gyrus (Obsessions, Compulsions and emotional regulation)
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Wed Sep 02, 2015 7:06 pm
Admin Wed Sep 02, 2015 7:06 pm
European Medicines Agency Released New Recommendations for Hydroxyzine (27 March 2015).
(1) Hydroxyzine has the potential to block hERG channels and other types of cardiac channels, resulting in a potential risk of QT interval prolongation and cardiac arrhythmia events (confirmed by clinical and post-marketing data)
(2) The potential risk of QT interval prolongation and torsades de pointes can therefore be adequately minimised through measures targeting the identified risk factors and restricting the use of hydroxyzine to the lowest effective dose for the shortest possible duration.
(3) The maximum dose in adults should be a total of 100 mg daily; in the elderly, if use cannot be avoided the maximum daily dose should be 50 mg.
(4) The maximum daily dose in children up to 40 kg in weight should be 2 mg/kg/day;
children over 40 kg should be given the adult dose.
(5) Use of hydroxyzine is contraindicated in patients with known acquired or congenital QT interval prolongation, or with a known risk factor for QT interval prolongation such as cardiovascular disease, significant electrolyte imbalance (hypokalaemia, hypomagnesaemia), family history of sudden cardiac death, significant bradycardia, or concomitant use of drugs known to prolong the QT interval and/or induce torsades de pointes.
(6) Use is not recommended in elderly patients, due to reduced elimination of hydroxyzine in these patients and greater vulnerability to anticholinergic effects and other adverse reactions.
(7) The medicine should be used with caution in patients with bradycardia, or who are taking hypokalaemia-inducing medicines.
(
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Wed Sep 02, 2015 7:12 pm
Admin Wed Sep 02, 2015 7:12 pm
Major depressive disorder is differentiated from bereavement by presence of:
- Suicidal ideations
- Sustained psychotic symptoms (not transient)
- Self deprecating thoughts
- Feelings of worthlessness and hopelessness.
Source: Lamb K, Pies R, Zisook S. The Bereavement Exclusion for the Diagnosis of Major Depression: To be, or not to be. Psychiatry (Edgmont). 2010 Jul;7(7):19-25.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Wed Sep 02, 2015 7:16 pm
Admin Wed Sep 02, 2015 7:16 pm
Identifying Dementia patient at risk of unsafe Driving
For patients with dementia, consider the following characteristics useful for identifying patients at increased risk for unsafe driving (Strength of evidence: A, B &C- Level A being highest and Level C is lowest strength of evidence)
• The CDR scale (Level A)
• A caregiver’s rating of a patient’s driving ability as marginal or unsafe (Level B)
• A history of traffic citations (Level C)
• A history of crashes (Level C)
• Reduced driving mileage (Level C)
• Self-reported situational avoidance (Level C)
• MMSE scores of < 24 (Level C)
• Aggressive or impulsive personality characteristics (Level C).
Patients with mild dementia (CDR of 1) are at a substantially higher risk for unsafe driving and thus should strongly consider discontinuing driving. The ORDT (On Road Driving Test) pass rate is 41-76% for CDR score of 1.
Source: Practice Parameter update: Evaluation and management of driving risk in dementia. Neurology 2010;74:1316–1324.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Wed Sep 02, 2015 7:20 pm
Admin Wed Sep 02, 2015 7:20 pm
Alzheimer's disease: Early onset vs Late onset.
* Familial (Early Onset) Alzheimer's disease: different single gene mutations on chromosomes 21, 14 and 1.
Mutation on Chromosome 21: abnormal Amyloid Precursor Protein (APP) formation.
Mutation on Chromosome 14: abnormal Presenilin 1.
Mutation on Chromosome 1: abnormal Presenilin 2.
* Late Onset Alzheimer's disease: increase risk related to Apolipoprotein E (APOE) gene- found on chromosome 19.
APOE e2: rare and may provide protection against the disease.
APOE e3: most common allele, play neutral role.
APOE e4: patient who develop Alzheimer's disease are more likely to have APOE e4.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Wed Sep 02, 2015 9:11 pm
Admin Wed Sep 02, 2015 9:11 pm
Medications for Alcohol Dependence
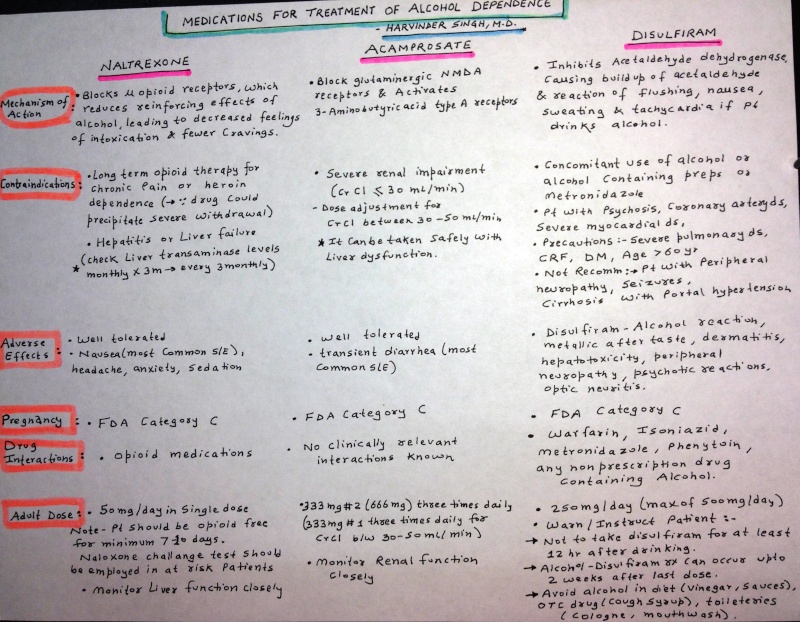
Naltrexone for Alcohol Dependence
- Primarily for more complex and severely dependent patients (note: high alcoholism risk is associated with LOW b-endorphin levels)
- Mechanism of action:
(a) Naltrexone raises b-endorphin (through feedback inhibition) via PRESYNAPTIC opioid receptors.
(b) Naltrexone reduces alcohol stimulation and craving by maximal b-endorphin stimulation of POSTSYNAPTIC u-opioid receptors.
(c) By this above mechanism b-endorphin levels are maximized --> alcohol cannot further raise b-endorphin OR increase u-opioid receptor stimulation --> thereby reducing “high” and priming effect from alcohol.
Last edited by Admin on Sat Sep 05, 2015 2:21 pm; edited 1 time in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -

Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 1:57 pm
Admin Sat Sep 05, 2015 1:57 pm
Level of Evidence for Antidepressant in Treating or Preventing Depression Emerging During HCV (Hepatitis C) Treatment
Level of Evidence and included medications:
Level I (≥ 2 RCTs or meta-analysis): only Escitalopram currently has Level 1 evidence for treating or preventing depression emerging during HCV treatment.
Level 2 (1 RCT): Citalopram and Paroxetine
Level 4 (Case reports/series or expert opinion): Bupropion, Fluoxetine, Sertraline, Mirtazapine, Venlafaxine, Desvenlafaxine, TCA
AVOID: Duloxetine and Nefazodone
Source: Sockalingam et al. BMC Gastroenterology 2013, 13:86.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 2:13 pm
Admin Sat Sep 05, 2015 2:13 pm
Narcolepsy with Cataplexy: Treatment.
- Sodium Oxybate is only FDA medication indicated for both Excessive Sleepiness and Cataplexy in Narcolepsy.
- Modafinil and Stimulants are FDA approved for Excessive Sleepiness (not Cataplexy) in Narcolepsy.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 2:15 pm
Admin Sat Sep 05, 2015 2:15 pm
Bipolar I vs ADHD in Children:
Following symptoms are more prominent in children with bipolar disorder-I, compared with those with only ADHD:
- Elevated Mood
- Grandiosity
- Flight of Ideas
- Decreased need for sleep
- Hypersexuality
Presence of following symptoms did not differentiate these two disorder:
- Irritability
- Accelerated speech
- Distractibility
Source:
- Psychiatric Annals Vol 44 NO 9 2014
- J Affect Disord. 1998;51 (2):81-91
Treatment of ADHD and Comorbid Bipolar Disorder
- Treat bipolar symptoms first, if ADHD symptoms persist, titrate medications carefully
- It may be safe to use stimulants if bipolar symptoms responded well to a mood-stabilizing agent
- Some evidence suggests that atomoxetine can be used safely and effectively in combination with mood stabilizers
- Stimulant use requires ongoing monitoring as it may destabilize the mood disorder
- Positive or negative response to a trial with a stimulant medication should not be used as a diagnostic tool in the process of differential diagnosis.
Last edited by Admin on Sat Sep 05, 2015 2:27 pm; edited 1 time in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 2:17 pm
Admin Sat Sep 05, 2015 2:17 pm
Factitious Disorders Management Recommendations:
(a) A comprehensive psychiatric assessment should be completed to identify comorbid psychiatric illnesses, and suicide risk.
(b) One person should have primary therapeutic responsibility.
(c) The multidisciplinary team should be involved with all being aware of the psychiatric assessment, risk assessment and treatment plan.
(d) If confrontation takes place, this should be non-punitive and supportive in nature.
(e) A treatment plan should be individualised to the patient.
(f) Comorbid illnesses should be treated appropriately.
(g) Long-term therapy or support should be provided to aid recovery and transition back into a ‘normal’ life.
Source: Psychother Psychosom 2008;77:209–218.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 2:23 pm
Admin Sat Sep 05, 2015 2:23 pm
Treatment of Persistent Aggressive Behaviors in Schizophrenia:
- Second-generation antipsychotics (best evidence): Clozapine > Olanzapine > Haloperidol
- Beta-blockers (second-best evidence)
- Mood stabilizers (weak evidence)
- Antidepressants (weak evidence)
- Benzodiazepines (negative evidence)
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 2:25 pm
Admin Sat Sep 05, 2015 2:25 pm
Bipolar disorder type II vs Borderline Personality Disorder
Factors Suggesting Bipolar Disorder type II:
Family history of bipolar disorder or major mood disorder
Clear onset
Failure to remit
Melancholic, agitated and mixed features when depressed
Uncharacteristic euphoria, creativity, grandiosity
Autonomous mood swings
Response to mood stabilizers
Increased rate of ADHD
Factors Suggesting Borderline Personality Disorder:
Family history of antisocial personality disorder, substance use disorder and unipolar depression.
Depressed entire life
Attenuated over time
Blames others. Cognitive symptoms of depression
Reactive moods, generally triggered by interpersonal events
Impulsivity to manage negative affect
Rarely remits on mood stabilizers
Non-Differentiating Factors:
Atypical features
Suicidality and self mutilation
Childhood trauma
Co-morbidity with anxiety and substance use disorders
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 2:30 pm
Admin Sat Sep 05, 2015 2:30 pm
Management of Behavioral and Psychological Symptoms of Dementia
- Atypical antipsychotics are first-line for emergencies (out of control patient) to prevent harm to patient/others
- If patient is psychotic, determine lowest maintenance dose of preferred agent
- Always discuss risk/benefit ratio of using atypicals with family/caregivers and document in chart
- If atypicals are required for tranquilization, always attempt prompt weaning and discontinuation
- If atypicals are used for psychosis, consider 12-month treatment before attempt at weaning/discontinuation
- Calming antidepressants such as trazodone may be useful for mild agitation
- Calming antidepressants such as citalopram may useful for agitation associated with depression
- Anticonvulsants such as oxcarbazepine and divalproex may be useful for impulsive aggressive behaviors; levetiracetam, gabapentine, and lamotrigine are not useful for agitation/aggressivity
- Sexually aggressive behaviors may respond to the anti-libidinal effects of SSRIs, or in severe cases, to conjugated estrogen or medroxyprogesterone
- As with all pharmacotherapies in the elderly, “start low and go slow”
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Page 1 of 3 • 1, 2, 3 ![]()
» prite exam
» Best Clinical Manual For "Mental Status Exam" ?
» Child & Adolescent Neuropsychiatric Mental Status Exam
» Updates from 2015 NEI Congress
FORUM FOR PSYCHIATRY RESIDENTS :: Psychiatry :: Psychiatry-Neurology-Psychology discussion :: Psychiatry In Depth
» L-Methylfolate: Who Will benefit
» Vitamins & Supplements in Clinical Practice.
» Imaging Biomarkers for Outcomes in Mild TBI
» Q.5 Clozapine Neutopenia
» Treating Disorders!
» Cortical Abnormalities in Adults & Adolescents with MDD
» Efficacy of Antipsychotics in Pediatric Acute Mania
» Obsessive Compulsive Disorder in Adults: Which Treatment is Better?