

The newest registered user is raheelmemon
Our users have posted a total of 1140 messages in 613 subjects

ABPN Initial Certification Exam 2015
FORUM FOR PSYCHIATRY RESIDENTS :: Psychiatry :: Psychiatry-Neurology-Psychology discussion :: Psychiatry In Depth
Page 2 of 3 •  1, 2, 3
1, 2, 3 ![]()
ABPN Initial Certification Exam 2015
![]() Admin Sat Aug 29, 2015 8:28 pm
Admin Sat Aug 29, 2015 8:28 pm

This thread is dedicated to ABPN (American Board of Psychiatry and Neurology) Initial Certification Exam 2015.
Exam Date: September 24-25, 2015
High yield topics will be posted here frequently over the course of next 1 month.
Index
Page 1:
1. Adjunctive use of Antidepressants for Bipolar Disorder (per recent ISBD Guidelines).
2. Lithium Facts (Not indicated in; Contraindications; Medications increasing/decreasing level; association with kidney function & thyroid).
3. Medications associated with symptoms of restless legs syndrome.
4. REM Sleep Changes in Depression.
5. Antipsychotics least likely to exacerbate OCD symptoms in patients with comorbid OCD and schizophrenia.
6. Neurochemical Abnormalities in Catatonia.
7. Neuropsychiatric Complications of Glucocorticoid Use.
8. Antipsychotics Effect on Prolactin levels in patients with breast cancer.
9. What is the Difference Between Amphetamine and Methylphenidate?
10. ECT and Contraindications.
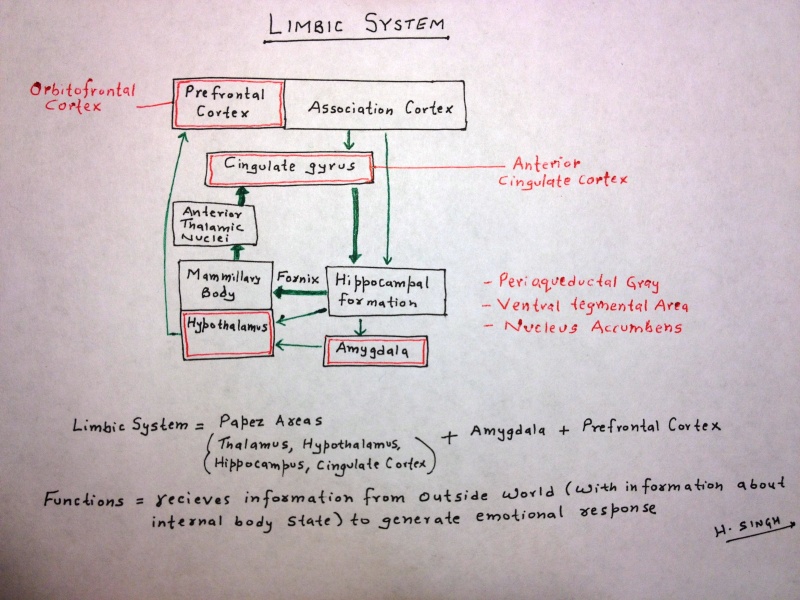
11. Brain structures involved in Anxiety.
12. New Recommendations for Hydroxyzine (European Medicines Agency).
13. Major depressive disorder vs bereavement.
14. Identifying Dementia patient at risk of unsafe Driving.
Page 2:
15. Alzheimer's disease: Early onset vs Late onset.
16. Medications for Alcohol Dependence + Naltrexone Mechanism.
17. Aphasia types.
18. Antidepressant in Treating or Preventing Depression Emerging During HCV (Hepatitis C) Treatment.
19. Narcolepsy with Cataplexy: Treatment
20. Bipolar I vs ADHD in Children + Treatment of ADHD and Comorbid Bipolar Disorder.
21. Factitious Disorders Management Recommendations.
22. Treatment of Persistent Aggressive Behaviors in Schizophrenia.
23. Bipolar disorder type II vs Borderline Personality Disorder.
24. Management of Behavioral and Psychological Symptoms of Dementia.
25. Donepezil, Rivastigmine & Galantamine: Use in Renal and Hepatic Impairment.
26. Mechanism of action of medications approved for weight loss.
27. Flibanserin Contraindications.
28. Antipsychotic Drug Use and the Risk of Seizures.
29. Rates of Placental Passage of Antipsychotics.
Page 3:
30. Treatment Options of Sexually Inappropriate Behavior in Dementia.
31. Acute Stress Disorder and Psychological debriefing.
32. Sleep Changes in Children and Elderly.
33. Personality Disorder and Defense Mechanisms
34. Neuro-Oncology: Important Histopathology Findings.
35. Basal Ganglia Structures and Diseases Associated with Damage.
36. Hippocampal Formation changes in Schizophrenia.
37. Antipsychotics least likely to increase QTc interval.
38. Model of Opioid Dysfunction and Buprenorphine Treatment in Borderline Personality Disorder.
39. Juvenile Myoclonic Epilepsy.
40. Poor & Good Prognostic Factors in Conversion Disorder.
41. Important EEG Findings.
42. Intellectual Disability Common Causes.
43. Anorexia Nervosa & Metabolic Abnormalities.
44. Pedophilic Disorder: Good and Bad Prognosis Indicators
Page 4:
45. Psychodynamic themes in Panic Disorder.
46. Sleep Stages & EEG Findings.
47. Postulated brain regions involved in different symptoms of ADHD.
48. Foods Avoided with MAOIs.
49. fMRI and Postmortem biopsy findings in Depression.
50. Antidepressants & False Positive Screen for Amphetamine.
51. FDA Approved Medications for Sleep Disorders.
52. Visual developmental milestones.
53. Children developmental milestones (important).
54. Psychopharmacology: Important CYP450 Interactions (*)
55. Incidence Rate and Period Prevalence.
56. Biostatistics.
57. Visual Pathway And Associated Visual Defects.
57. Peripheral Nerves: Radial, Ulnar, Median and Musculocutaenous.
58. Drug of Choice for Psychosis in Parkinson's Disease.
Page 5:
60. Erikson's stages of psychosocial development.

Last edited by Admin on Sat Sep 19, 2015 8:07 pm; edited 54 times in total

Admin- Admin

- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -

Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 2:33 pm
Admin Sat Sep 05, 2015 2:33 pm
Donepezil, Rivastigmine & Galantamine: Use in Renal and Hepatic Impairment.
Donepezil:
* Single doses of donepezil can be safely administered to patients with moderately to severely impaired renal function (creatinine clearance < 30 ml/ min)
* Multiple doses can be safely administered to patients with moderately impaired renal function (creatinine clearance 17–33 ml/min)
* Multiple-dose studies of donepezil in patients with hepatic impairment (not to exceed Grade B as defined by the Child-Pugh Classification) indicate that donepezil 5 mg/day is a safe and well-tolerated treatment.
Source: Br J Clin Pharmacol. Nov 2004; 58(Suppl 1): 1–8.
Rivastigmine:
* In patients with moderate to severe renal impairment (glomerular filtration rate <50 mL/min), clearance of oral rivastigmine was reduced. Accordingly, such patients may be able to only tolerate lower doses.
* In patients with mild or moderate hepatic impairment (Child-Pugh score 5 to 9), clearance of oral rivastigmine was reduced. Accordingly, such patients may be able to only tolerate lower doses.
* No data are available on the use of rivastigmine in patients with severe hepatic impairment.
Source: Rivastigmine Package Insert
Galantamine:
* Use with caution in patients with mild-to-moderate liver impairment; not recommended in severe impairment.
* Use with caution in patients with moderate renal impairment; not recommended in severe impairment (CrCl <9 mL/minute).
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 2:38 pm
Admin Sat Sep 05, 2015 2:38 pm
Mechanism of action of medications approved for weight loss:-
Lorcaserin —> stimulates 5HT2C receptor —> stimulates POMC neuron —-> releases alpha MSH —> acts on MC4R —> resulting in suppression of appetite
Phentermine —> increases NE and Dopamine at POMC neuron —-> releases alpha MSH —> acts on MC4R —> resulting in suppression of appetite
Topiramate —> increases GABA and decreases Glutamate on AgRP/NPY neuron —> decreases release of AgRP/NPY —> no longer stimulation of appetite —> decreased appetite
Phentermine + Topiramate —> additive effects
Bupropion—> increases NE and Dopamine at POMC neuron —-> releases alpha MSH —> acts on MC4R —> resulting in suppression of appetite
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 2:48 pm
Admin Sat Sep 05, 2015 2:48 pm
Flibanserin Contraindications:
Flibanserin is indicated for the treatment of premenopausal women with acquired, generalized hypoactive sexual desire disorder.

Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 2:52 pm
Admin Sat Sep 05, 2015 2:52 pm
Antipsychotic Drug Use and the Risk of Seizures.
Methods: UK-based Clinical Practice Research Datalink database to conduct a follow-up study with a nested case-control analysis between 1998 and 2013.
Results:
(a) Incidence rate of seizures per 10,000 person-years was:
- Olanzapine or Quetiapine = 32.6,
- Amisulpride, Aripiprazole, Risperidone, or Sulpiride= 24.1
- Low-to-Medium Potency Antipsychotic= 49.4
- Medium-to-High Potency Antipsychotic= 59.1
- Non-Users of Antipsychotic= 11.7
(b) Patients with dementia had significantly higher incidence rates of first-time seizures compared with patients with affective disorders, irrespective of antipsychotic drug use.
(c) In patients with affective disorders:
- Current use of medium-to-high potency first-generation antipsychotic drugs was associated with an increased risk of seizures compared with non-use.
- Use of other antipsychotic drugs was not associated with seizures.
(d) In patients with dementia:
- Current use of olanzapine or quetiapine, low-to-medium potency first-generation antipsychotic drugs, and medium-to-high potency first-generation antipsychotic drugs was associated with an increased risk of seizures compared with non-use,
- Current use of amisulpride, aripiprazole, risperidone, or sulpiride was not associated with an increased risk of seizures.
CNS Drugs. 2015 Aug 5.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 2:56 pm
Admin Sat Sep 05, 2015 2:56 pm
Rates of Placental Passage of Antipsychotics:
Olanzapine > Risperidone > Quetiapine
Quetiapine is a reasonable first choice when a new atypical antipsychotic is indicated for a pregnant patient. In clinical trials, quetiapine had lower rates of placental passage compared with risperidone and olanzapine.
Source: Am J Psychiatry. 2007;164(
Prospective studies show no increase in fetal malformations or adverse neonatal health outcomes with quetiapine.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 2:58 pm
Admin Sat Sep 05, 2015 2:58 pm
Treatment Options of Sexually Inappropriate Behavior in Dementia
* The most common individual treatment choices were haloperidol (15%), thioridazine (11%), and risperidone (10%).
* SSRIs can cause sexual dysfunction as a side effect and may offer additional benefits for other behavioral symptoms.
The antidepressants paroxetine, citalopram, clomipramine and fluoxetine have been used, with citalopram being the most commonly prescribed of these drugs.
* The anticonvulsant drugs carbamazapine and gabapentine, which are the only two anticonvulsants reportedly used with favorable results.
* One case report of pindolol, a beta blocker, where Pindolol completely eliminate this behavior in 2 weeks.
* Cimetidine is a H2 receptor antagonist and also has antiandrogen effects. It blocks the androgen receptor in the pituitary or the hypothalamus, reducing sexual desire in individuals of both sexes and affecting arousal and orgasm.
Source: Annals of Long-Term Care: Clinical Care and Aging. 2015;23(6):39-42.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 5:11 pm
Admin Sat Sep 05, 2015 5:11 pm
Acute Stress Disorder and Psychological debriefing.
Psychological debriefing was developed as an intervention to prevent the development of negative emotional consequences of trauma including Acute Stress Disorder, but well controlled studies using single-session individual or group debriefings have not demonstrated efficacy.
So Psychological debriefing is not Recommended as treatment for Acute Stress Disorder.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Sat Sep 05, 2015 10:36 pm
Admin Sat Sep 05, 2015 10:36 pm
Sleep Changes in Children and Elderly

Compared with young adults, the elderly tend to have:
- delayed sleep onset,
- fragmented sleep,
- early-morning awakening,
- decreased time in sleep stages 3 and 4.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Mon Sep 07, 2015 12:05 pm
Admin Mon Sep 07, 2015 12:05 pm
Personality Disorder and Defense Mechanisms
1. Obsessive Compulsive:
* Isolation of Affect
* Reaction Formation
* Intellectualization
* Rationalization
* Undoing
2. Borderline:
* Splitting
* Projective Identification
* Denial
* Distortion
* Dissociation
3. Antisocial:
* Projection
* Projective Identification
* Acting out
* Somatization
* Isolation of Affect
* Dissociation
4. Histrionic:
* Sexualization
* Repression
* Regression
* Displacement
* Conversion
* Dissocation
5. Paranoid:
* Projection
* Denial
6. Schizoid:
* Schizoid Fantasy
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Mon Sep 07, 2015 12:16 pm
Admin Mon Sep 07, 2015 12:16 pm
Neuro-Oncology: Important Histopathology Findings:
* Pilocytic Astrocytomas (Grade I): Rosenthal fibers (beaded, elongated, or corkscrew-shaped intracytoplasmic inclusions).
* Glioblastoma Multiforme (Grade IV): "Pseudopalisading" Necrosis.
* Oligodendrogliomas: Fried egg appearance (round cells with perinuclear halo).
* Ependymomas: Perivascular pseudorosettes and ependymal rosettes.
* Medulloblastoma: small round blue cells.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Mon Sep 07, 2015 12:18 pm
Admin Mon Sep 07, 2015 12:18 pm
Basal Ganglia Structures and Diseases Associated with Damage.

Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Mon Sep 07, 2015 12:21 pm
Admin Mon Sep 07, 2015 12:21 pm
Hippocampal Formation changes in Schizophrenia.

Reduced glutamatergic transmission in the dentate gyrus is the basis for "reduced pattern separation" function in schizophrenia and, furthermore, serves to generate an "increase in long-term potentiation" in CA3 and "greater pattern completion" function, including the production of psychotic thoughts and the encoding of the psychotic productions as normal memory. i.e., during a novel experience, the schizophrenic hippocampus may erroneously retrieve a memory of a past event rather than appropriately encode a new distinct memory representation.
Source: Am J Psychiatry 167:10, October 2010
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Mon Sep 07, 2015 12:24 pm
Admin Mon Sep 07, 2015 12:24 pm
Antipsychotics least likely to increase QTc interval:
* Lurasidone
* Aripiprazole
* Paliparidone
* Asenapine
Source: Lancet. 2013 Sep 14;382(9896):951-62
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Mon Sep 07, 2015 12:28 pm
Admin Mon Sep 07, 2015 12:28 pm
Model of Opioid Dysfunction and Buprenorphine Treatment in Borderline Personality Disorder:
* Basal opioid levels in borderline personality disorder are hypothesized to be reduced in output, while receptors are increased in number, so that during unstimulated conditions, borderline patients experience dysphoria associated with reduced tonic opioid activity.
* When stress or pain causes an increase in release of opioids, there is an increased opioid signal and relief from dysphoria.
Treatment with Buprenorphine, a partial agonist, would:
* Increase basal opioid signal under baseline conditions of low tonic activity and
* Antagonize opioid receptors under conditions of increased output (e.g., self-injurious behavior).
Note:
Buprenorphine:
* partial agonist at mu-opioid receptor.
* antagonist at kappa-opioid receptor.
Naloxone:
* antagonist at the mu-opioid receptor.
Source: Am J Psychiatry. 2009;167(1):24-39
Last edited by Admin on Sun Sep 13, 2015 8:55 pm; edited 1 time in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Mon Sep 07, 2015 12:30 pm
Admin Mon Sep 07, 2015 12:30 pm
Juvenile Myoclonic Epilepsy (JME)
* Patients have normal intelligence with onset around adolescence and has a family history of JME.
* Seizures occur shortly after awakening or after precipitating factors such as sleep deprivation, alcohol use, or psychological stress.
* The study of choice for confirming the clinical diagnosis is sleep-deprived EEG with activation procedures (ie, hyperventilation, photic stimulation).
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Mon Sep 07, 2015 12:33 pm
Admin Mon Sep 07, 2015 12:33 pm
Prognostic Factors in Conversion Disorder:
Poor prognostic symptoms:
* Pseudoseizure (psychogenic nonepileptic seizure)
* Psychogenic tremor
* Subclinical (undiagnosed) personality pathology
* Presence of a stuffed animal brought to the hospital by the patient
* Poor perception of own well-being
* Pending litigation
Good prognostic factors:
* Acute onset of symptoms
* Short duration of symptoms
* Healthy premorbid functioning
* Higher intelligence
* Absence of coexisting psychopathology
* Presence of an identifiable stressor
* Male gender
* Change in marital status (marriage or divorce)
* Isolated sensory symptoms
* Very young age
* Good premorbid medical health status.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Mon Sep 07, 2015 1:53 pm
Admin Mon Sep 07, 2015 1:53 pm
Important EEG Findings:
1. Hepatic Encephalopathy: diffuse slowing.
2. Alcohol or sedative withdrawal: increased fast wave activity.
3. Metabolic or Toxic Delirium: triphasic waves.
4. Focal Lesions: localized delta waves.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Mon Sep 07, 2015 3:39 pm
Admin Mon Sep 07, 2015 3:39 pm
Intellectual Disability Common Causes:
* Most common genetic cause = Down's Syndrome
* Most common inherited cause = Fragile X Syndrome
* Most common preventable cause = Fetal alcohol syndrome
Last edited by Admin on Sun Sep 13, 2015 4:05 pm; edited 1 time in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Mon Sep 07, 2015 8:44 pm
Admin Mon Sep 07, 2015 8:44 pm
Anorexia Nervosa & Metabolic Abnormalities:
* Anorexia Nervosa, Laxative abuse = Hyponatremia, Hyperchloremic Metabolic Acidosis.
* Anorexia Nervosa, Vomiting = Hypokalemic, Hypochloremic Metabolic Alkalosis.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Wed Sep 09, 2015 8:21 pm
Admin Wed Sep 09, 2015 8:21 pm
Pedophilic Disorder: Good and Bad Prognosis Indicators:
Bad Prognosis Indicators:
1. Early age of onset
2. Higher frequency of acts
3. Lack of guilt
4. Antisocial personality disorder (ASPD)
5. Substance abuse presence
6. Referred by legal agency
Good Prognosis Indicators:
1. Single Paraphilic disorder presence
2. Intelligence normal
3. No substance abuse
4. No ASPD
5. History of normal intercourse in additional to paraphilic disorder
6. self referred
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Wed Sep 09, 2015 8:33 pm
Admin Wed Sep 09, 2015 8:33 pm
Psychodynamic themes in Panic Disorder:
(a) Internal representations of relationships involving sexual or physical abuse.
(b) Vicious cycle of anger at parental rejecting behavior followed by anxiety that fantasy will destroy the tie to parents.
(c) Typical defense mechanisms include reaction formation, undoing and externalization.
(d) Failure of signal anxiety function in ego related to self fragmentation and self-other boundary confusion.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Wed Sep 09, 2015 8:39 pm
Admin Wed Sep 09, 2015 8:39 pm
Sleep Stages & EEG Findings:
Stage I: Theta activity (3-7 cps)
Stage II: Negative sharp wave followed by positive sharp waves= K complexes
Stage III: Delta waves (high amplitude, slow waves < 2cps) occupying 20-50%
Stage IV: Delta waves occupy >50%
REM: Saw tooth waves
Sleep begins in Stage 1 and progresses into stages 2, 3, and 4. However Sleep does not progress through all of these stages in sequence. Then, after Stage 4 sleep, Stages 3, then 2 are repeated before going into REM sleep. We typically enter REM approximately 90 minutes after falling asleep. The first cycle of REM is shortest (usually lasting 10 mins), but with each cycle REM becomes longer (15-40 min each). Once REM is over, we usually return to Stage 2 sleep.
In general, there are four to six cycles of NREM sleep per night, which are followed by brief intervals of REM sleep.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Wed Sep 09, 2015 8:47 pm
Admin Wed Sep 09, 2015 8:47 pm
Postulated brain regions involved in different symptoms of ADHD:
1. Inattention Symptoms: Dorso-Lateral Prefrontal Cortex and Anterior Cingulate Cortex
2. Hyperactivity Symptoms: Prefrontal motor cortex
3. Impulsive symptoms: Orbital frontal cortex.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Wed Sep 09, 2015 8:49 pm
Admin Wed Sep 09, 2015 8:49 pm
Foods Avoided with MAOIs:
* Among Milk and Diary products:
- All aged cheeses are to be avoided. Tyramine content increases as the cheese ages.
* Among Fruits and Vegetables:
- should be fresh and not overripe or spoiled.
- Avoid broad bean pods
* Breads:
- Brewer's yeast is rich in tyramine content so avoid
* Meat and other protein source:
- All meats, fish and poultry are safe if fresh or frozen.
- Avoid all dried, salted or smoked products.
- Avoid if canned or greater than five days old.
- Cooking does not destroy tyramine content.
* Alcohol:
- Avoid tap and unpasturaized beers
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: ABPN Initial Certification Exam 2015
![]() Admin Wed Sep 09, 2015 8:52 pm
Admin Wed Sep 09, 2015 8:52 pm
In Depression fMRI and Postmortem biopsy studies consistently show
(A) Increased Volume and Gray Matter in:
- Amygdala
- Insula
(B) Decreased Volume and Gray Matter in:
- Prefrontal Cortex
- Hippocampus
- Striatum
For overview on neurocircuitry:-
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Page 2 of 3 • 1, 2, 3 ![]()
» prite exam
» Child & Adolescent Neuropsychiatric Mental Status Exam
» Best Clinical Manual For "Mental Status Exam" ?
» Updates from 2015 NEI Congress
FORUM FOR PSYCHIATRY RESIDENTS :: Psychiatry :: Psychiatry-Neurology-Psychology discussion :: Psychiatry In Depth
» L-Methylfolate: Who Will benefit
» Vitamins & Supplements in Clinical Practice.
» Imaging Biomarkers for Outcomes in Mild TBI
» Q.5 Clozapine Neutopenia
» Treating Disorders!
» Cortical Abnormalities in Adults & Adolescents with MDD
» Efficacy of Antipsychotics in Pediatric Acute Mania
» Obsessive Compulsive Disorder in Adults: Which Treatment is Better?