

The newest registered user is raheelmemon
Our users have posted a total of 1140 messages in 613 subjects

PRITE High Yield Topic Discussion Thread
FORUM FOR PSYCHIATRY RESIDENTS :: Psychiatry :: Psychiatry-Neurology-Psychology discussion :: Psychiatry In Depth
Page 2 of 4 •  1, 2, 3, 4
1, 2, 3, 4 ![]()
PRITE High Yield Topic Discussion Thread
![]() Admin Sun Sep 04, 2011 9:45 pm
Admin Sun Sep 04, 2011 9:45 pm
Hi Friends.
This thread is dedicated to PRITE (Psychiatry Resident-In-Training Examination) Preparation.
Please contribute important high yield topics and notes here.

INDEX:
Page 1:
• Typical Antipsychotics
• Borderline Personality Disorder
• Schizophrenia
• Dopaminergic Pathway Functions & Effect of Antipsychotics
• Sigmund Freud’s Structural Model- The id, ego, and superego
• Major depression with Atypical features
• Akathisia treatment
• Rabbit Syndrome
• Risperidone vs Clozapine
Page 2:
• Cluster A Personality disorder- differential diagnosis
• Cluster B Personality disorder- differential diagnosis
• Cluster C Personality disorder- differential diagnosis
• Personality disorder in toto (HY Facts)
• Frontotemporal dementia Vs Alzheimer’s dementia
• Autoreceptors Vs Heteroreceptors
• Visual Pathway And Associated Visual Defects
• Myasthenia Gravis
• Jean Piaget's Cognitive Development Stages
• Normal Aging- Facts
• Erikson's Stages of Psychosocial Development
• Cognitive Theory for depression Management
Page 3:
• Interpersonal Therapy (IPT)
• Valproate
• Childhood Onset Schizophrenia
• Recommendations for monitoring adults on atypical antipsychotics
• Pediatric Depression- Which SSRI is Superior
• Neuroleptic Malignant Syndrome
• Hispanic culture-bound syndromes
• Elevated Clozapine Levels
• Pervasive Developmental Disorder Not Otherwise Specified (Including Atypical Autism)
• Diagnostic criteria for Attention-Deficit/Hyperactivity Disorder
• Diagnostic criteria for Gender Identity Disorder
• Freud's Topographical Model
• HIV Dementia/Toxoplasmosis/CNS Lymphoma/Cryptococcal Meningitis/PML
• Gait Abnormalities
Page 4:
• Trigeminal neuralgia Vs Post Herpetic Neuralgia
• Carbon Monoxide Toxicity: Brain MRI Findings
• Lumbar & Sacral Nerve Root Compromise
• Classic Conditioning Vs Operant Conditioning
• Observational Study Design: Case control Vs Cohort
• Alexia/Apraxia/Agnosia/Akinesia/Aphasia
• Adjustment Disorders Vs Acute Stress Disorder
• SNRIs: Venlafaxine Vs Duloxetine
• DSM IV Criteria for Manic Episode
• Bipolar Disorder: 15 Minutes CORE Psychiatric Evaluation- 4 Decision Points
• Bipolar Depression Vs Unipolar Depression
• Difference Between Classical Conditioning & Extinction
• "Neurology" Questions/HY Facts for PRITE (Post 1 & 2)
Page 5:
• Catatonia
• CVA
• "Delirium" & "Dementia"
• Seizure
• Obsessive-compulsive disorders
• Role of Ziprasidone in combination therapy for Bipolar maintenance
• Recognition of GAD in Primary Care Setting
• Social Anxiety Disorder
• Panic Disorder
• ADHD (Recent Facts)
• Basics of Nor-Epinephrine, Dopamine & Seretonin Neurons.
• Hyperprolactinaemia With Antipsychotics
• Idiopathic Parkinson Ds Vs Other Parkinsonian Syndrome
• Pathophysiology of Neuroleptic Malignant Syndrome (NMS)
Page 6:
• Treatment of Juvenile Myoclonic Epilepsy
• Borderline Personality Disorder- What Questions to Ask?
• Transient Global Amnesia- Facts.
• Effective Dose for Antipsychotics- ED50 & Near-Maximal ED
• Fatal Familial Insomnia
• Medications for Alcohol Dependence
• Serotonin Toxicity- Diagnostic Criteria
• Alexithymia
• AACAP Practice Parameters for Bipolar Disorder in Children
• Progressive Supranuclear Palsy Vs Parkinson's disease
• Treatment of Depression with Atypical Features
• Types of Aphasia
• The Social Learning Theory of Julian B. Rotter
***** Updated Daily *****
Regards
Administrator
Last edited by Admin on Sun Nov 24, 2013 7:29 pm; edited 67 times in total

Admin- Admin

- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -

Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sat Sep 10, 2011 1:27 am
Admin Sat Sep 10, 2011 1:27 am
- ACh neuro-muscular transmission is impaired in Myasthenia, but ACh transmission in CNS is normal- illustrated by profound weakness but normal cognitive capacity.
- Most AntiAChE Myasthenia medications have no effect on CNS ACh activity (as do not penetrate blood brain barrier)- Exception is Physostigmine, which crosses BBB
- Earliest clinical feature is Diplopia and/or Ptosis
- Extra-ocular muscles may be paretic, but intra-ocular muscles are spared (normal size pupil & normal reactivity to light)
Differential Diagnosis:
(1)
| Lesions of Cranial N III | Myasthenia Gravis |
| Pupil dilated & not reactive to light | normal size pupil & normal reactivity to light |
Management of Myasthenia Gravis:
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sat Sep 10, 2011 3:18 pm
Admin Sat Sep 10, 2011 3:18 pm
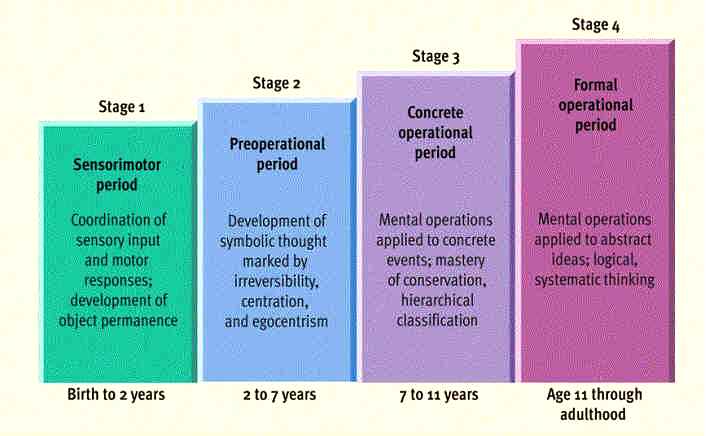
(1) Sensorimotor Stage (Birth to 2 Years)
- The critical achievement of this period is the development of Object permanence or the schema of the permanent object- Child's ability to understand that objects have an existence independent of the child's involvement with them. Infants learn to differentiate themselves from the world and are able to maintain a mental image of an object, even when it is not present and visible. When an object is dropped in front of infants, they look down to the ground to search for the object; that is, they behave for the first time as though the object has a reality outside themselves.
- The attainment of object permanence marks the transition from the sensorimotor stage to the preoperational stage of development.
- At about 18 months, infants begin to develop mental symbols and to use words, a process known as Symbolization. Infants are able to create a visual image of a ball or a mental symbol of the word ball to stand for, or signify, the real object. Such mental representations allow children to operate on new conceptual levels.
(2) Stage of Preoperational Thought (2 to 7 Years)
- Children in this stage have a sense of Immanent justice, the belief that punishment for bad deeds is inevitable.
- Children in this developmental stage are Egocentric: They see themselves as the center of the universe; they have a limited point of view; and they are unable to take the role of another person. Children are unable to modify their behavior for someone else; for example, children are not being negativistic when they do not listen to a command to be quiet because their brother has to study.
- During this stage, children also use a type of magical thinking, called Phenomenalistic Causality, in which events that occur together are thought to cause one another (e.g., thunder causes lightning, and bad thoughts cause accidents).
- Children use Animistic thinking, which is the tendency to endow physical events and objects with life-like psychological attributes, such as feelings and intentions.
- Semiotic Function: With this new ability, children can represent something- such as an object, an event, or a conceptual scheme-with a signifier, which serves a representative function (e.g., language, mental image, symbolic gesture). That is, children use a symbol or sign to stand for something else. Drawing is a semiotic function initially done as a playful exercise but eventually signifying something else in the real world.
(3) Stage of Concrete Operations (7 to 11 Years)
- Egocentric thought is replaced by Operational thought, which involves dealing with a wide array of information outside the child. Therefore, children can now see things from someone else's perspective.
- Syllogistic reasoning, in which a logical conclusion is formed from two premises, appears during this stage; for example, all horses are mammals (premise); all mammals are warm blooded (premise); therefore, all horses are warm blooded (conclusion).
- Conservation is the ability to recognize that, although the shape of objects may change, the objects still maintain or conserve other characteristics that enable them to be recognized as the same. For example, if a ball of clay is rolled into a long, thin sausage shape, children recognize that each form contains the same amount of clay. An inability to conserve (which is characteristic of the preoperational stage) is observed when a child declares that there is more clay in the sausage-shaped piece because it is longer.
- Reversibility is the capacity to understand the relation between things, to realize that one thing can turn into another and back again- for example, ice and water.
- The most important sign that children are still in the preoperational stage is that they have not achieved conservation or reversibility
(4) Stage of Formal Operations (11 through the End of Adolescence)
- Dealing with the future and its possibilities occurs in the formal operational stage
- Characterized by the ability to think abstractly, to reason deductively, and to define concepts and also by the emergence of skills for dealing with permutations and combinations
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sat Sep 10, 2011 8:32 pm
Admin Sat Sep 10, 2011 8:32 pm
- General intelligence declines slightly (measured by Weschler Adult Intelligence Scale Revised- WAIS-R)
- Shorter attention span, slower learning (acquisition of new knowledge), & decreased ability to perform complex tasks.
- Little or No loss of vocabulary, language ability, reading comprehension or general information.
Thus people older than 65 yr tends to remain well spoken, well read & knowledgeable, although somewhat forgetful.
- Sleep: fragmented sleep, less stage 4 NREM sleep, Delta wave amplitude decreases and proportionally less time is spent in stage 3 and stage 4 sleep.
- Senile gait
- EEG: slowing of normal background alpha activity (8-12 Hz)
- CT/MRI: Normal or decreased volumes of cerebral hemispheres, atrophy of cerebral cortex, expansion of sylvian fissure, and increased volume of lateral & third ventricle.
Also white matter hyper-intensities in many older peoples.
- Age associated histologic changes: Loss of large cortical neurons, presence of lipofuscin granules, granulovascular degeneration, senile plaques that contain amyloid and limited number of neurofibrillary tangles.
Last edited by Admin on Mon Sep 12, 2011 1:33 pm; edited 1 time in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sun Sep 11, 2011 2:36 pm
Admin Sun Sep 11, 2011 2:36 pm
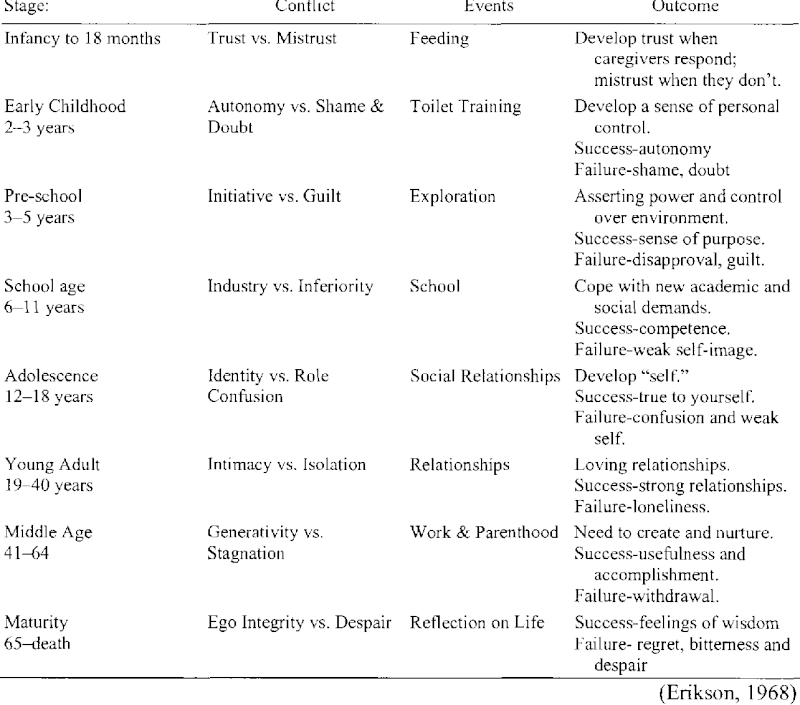
Psychosocial Stage 1 - Trust vs. Mistrust (Birth to about 18 Months)
- Because an infant is utterly dependent, the development of trust is based on the dependability and quality of the child’s caregivers.
- If a child successfully develops trust, he or she will feel safe and secure in the world.
- Caregivers who are inconsistent, emotionally unavailable, or rejecting contribute to feelings of mistrust in the children they care for. Failure to develop trust will result in fear and a belief that the world is inconsistent and unpredictable.
- A person who, as a result of severe disturbances in the earliest dyadic relationships, fails to develop a basic sense of trust or the virtue of hope may be predisposed as an adult to the profound withdrawal and regression characteristic of schizophrenia.
- Lack of trust responsible for:
* Dysthymic disorder, depressive disorders
* Paranoid & delusional disorder
* Schizoid personality disorder
* Substance related disorders
Psychosocial Stage 2 - Autonomy vs. Shame and Doubt (about 18 Months to about 3 Years)
- The second stage is focused on children developing a greater sense of personal control.
- Like Freud, Erikson believed that toilet training was a vital part of this process. However, Erikson's reasoning was quite different then that of Freud's. Erikson believe that learning to control one’s body functions leads to a feeling of control and a sense of independence.
- Other important events include gaining more control over food choices, toy preferences, and clothing selection.
- Children who successfully complete this stage feel secure and confident, while those who do not are left with a sense of inadequacy and self-doubt.
- A person who becomes fixated at the transition between the development of "hope" and "autonomous will", with its residue of mistrust and doubt, may develop paranoiac fears of persecution.
- Too rigorous toilet training, commonplace in today's society, which requires a clean, punctual, and deodorized body, can produce an overly compulsive personality that is stingy, meticulous, and selfish. Known as anal personalities, such persons are parsimonious, punctual, and perfectionistic (the three Ps).
- The ruminative and ritualistic behavior of the person who suffers from an obsessive compulsive disorder may be an outcome of the triumph of doubt over autonomy and the subsequent development of a primitively harsh conscience.
Psychosocial Stage 3 - Initiative vs. Guilt (about 3 Years to about 5 Years)
- During this stage, children begin to assert their power and control over the world through directing play and other social interaction.
- Children who are successful at this stage feel capable and able to lead others. Those who fail to acquire these skills are left with a sense of guilt, self-doubt and lack of initiative.
- When there has been an inadequate resolution of the conflict between initiative and guilt, the person may ultimately develop a conversion disorder, inhibition, or phobia.
- Those who overcompensate for the conflict by driving themselves too hard may experience sufficient stress to produce psychosomatic symptoms.
- Excessive guilt can lead:
* Generalized anxiety disorder
* Specific phobias
* Conversion Disorder
* May develop Psychosomatic disease
Psychosocial Stage 4 - Industry vs. Inferiority (about 5 Years to about 13 Years)
- Through social interactions, children begin to develop a sense of pride in their accomplishments and abilities.
- Children who are encouraged and commended by parents and teachers develop a feeling of "competence" and belief in their skills. Those who receive little or no encouragement from parents, teachers, or peers will doubt their ability to be successful.
- For some persons, the feelings may result in a compensatory drive for money, power, and prestige. Work can become the main focus of life, at the expense of intimacy.
Psychosocial Stage 5 - Identity vs. Confusion (about 13 Years to about 21 Years)
- During adolescence, children are exploring their independence and developing a sense of self.
- With the attainment of a more sharply focused identity, the youth develops the virtue of "Fidelity"- faithfulness not only to the nascent self-definition but also to an ideology that provides a version of self-in-world
- Those who receive proper encouragement and reinforcement through personal exploration will emerge from this stage with a strong sense of self and a feeling of independence and control. Those who remain unsure of their beliefs and desires will insecure and confused about themselves and the future.
- Erikson held that delinquency, gender-related identity disorders, and borderline psychotic episodes can result from such confusion.
Psychosocial Stage 6 - Intimacy vs. Isolation (about 21 Years to about 40 Years)
- Erikson believed it was vital that people develop close, committed relationships with other people. Those who are successful at this step will develop relationships that are committed and secure.
- Remember that each step builds on skills learned in previous steps. Erikson believed that a strong sense of personal identity was important to developing intimate relationships.
- Studies have demonstrated that those with a poor sense of self tend to have less committed relationships and are more likely to suffer emotional isolation, loneliness, and depression.
- "Distantiation", an awkward term coined by Erikson to mean "the readiness to repudiate, isolate, and, if necessary, destroy those forces and persons whose essence seems dangerous to one's own," is the pathological outcome of conflicts surrounding intimacy and, in the absence of an ethical sense where intimate, competitive, and combative relationships are differentiated, forms the basis for various forms of prejudice, persecution, and psychopathology.
- responsible for schizoid personality disorder
Psychosocial Stage 7 - Generativity vs. Stagnation (about 40 Years to about 60 Years)
- During adulthood, we continue to build our lives, focusing on our career and family.
- Those who are successful during this phase will feel that they are contributing to the world by being active in their home and community. Those who fail to attain this skill will feel unproductive and uninvolved in the world.
Psychosocial Stage 8 - Integrity vs. Despair (about 60 Years to Death)
- Those who are unsuccessful during this phase will feel that their life has been wasted and will experience many regrets. The individual will be left with feelings of bitterness and despair.
- Those who feel proud of their accomplishments will feel a sense of integrity. Successfully completing this phase means looking back with few regrets and a general feeling of satisfaction. These individuals will attain wisdom, even when confronting death.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() psychinmymind Sun Sep 11, 2011 9:41 pm
psychinmymind Sun Sep 11, 2011 9:41 pm
the future. Cognitive therapy seeks to identify these negative cognitions (sometimes called “hot thoughts”) and
replace them with healthier adaptive cognitions. This process frequently involves looking at the evidence that the
patient has found to support his/her negative cognition, developing more adaptive cognitions and looking at
evidence to support the more adaptive cognitions, and systematically helping the patient solidify the more adaptive
ways of thinking. Evidence indicates good efficacy of cognitive therapy in the treatment of mild depressions and its
positive role augmenting response to medication for acute treatment, as well as possibly preventing further episodes
in the future.
psychinmymind- Moderator

- Posts : 24
Points : 44
Reputation : 3
Join date : 2011-04-14
Location : Arizona
Re: PRITE High Yield Topic Discussion Thread
![]() psychinmymind Sun Sep 11, 2011 9:41 pm
psychinmymind Sun Sep 11, 2011 9:41 pm
relationships, communication, and socialization by addressing both present and past significant relationships.
Intrapsychic processes are less emphasized than in traditional psychoanalysis or psychodynamic therapy.
psychinmymind- Moderator
- Posts : 24
Points : 44
Reputation : 3
Join date : 2011-04-14
Location : Arizona
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sun Sep 11, 2011 9:50 pm
Admin Sun Sep 11, 2011 9:50 pm
(A) Particularly effective as a Prophylaxis in:
- Rapid cycling Bipolar disorder
- Dysphoric or Mixed mania
- Mania due to general medical condition
- Pt with comorbid substance use or panic attack
- not favorable response to Lithium
(B) Investigations indicated prior to starting Valproate:
CBC (White cell & Platelet count), and LFTs ----> Repeat at 1 month (if normal) ---> repeat every 6-14 months (if normal)
Mild increase in transaminases (< 3 times normal) ---> repeat every 1-2 week ---> if stable --> monitor every 3 monthly
Pronounced increase in transaminases (>3 times normal)+ symptomatic--->Reduce/ discontinue Valproate
Note: Asymptomatic elevation of transaminases >3 times normal, is common and do not require any changes in dosage.
(C) Risk factor for potential hepatotoxicity:
- Age <3 yr
- Concurrent use of phenobarbital
- Presence of neurologic disorders e.g., inborn error of metabolism or mental retardation.
Asymptomatic amylase elevation is not predictive of pancreatitis
Hyperammonemia with Valproate- common with Carbamazepine; S/S: Coarse Tremors; Responds to L-Carnitine
Thrombocytopenia with Valproate:
- Decrease dose if clinically symptomatic (bruising, bleeding gums)
- Most likely with Valproate level of: >110 (women) & >135 (men)
(D) if possible, Valproate should not be used in pregnancy- risk reduced with daily Folic acid (1-4 mg)
Not contraindicated in nursing mothers.
In adolescent & young females: cases of PCOD (Polycystic Ovary Disease)
(E) Most common adverse effects: GI (Nausea, Vomiting, Dyspepsia, & Diarrhea)
Valproate induced tremors: beta blockers, or gabapentin
Weight gain: Tt- Strict limitation of caloric intake
Higher dosage of Valproate (> 1000 mg/day)- moderate hyponatremia (SIADH)
(F) Drug Interactions:
- Valproate + Lamotrigine = doubles Lamotrigine levels -->risk of serious rash
- Valproate + Lithium = increased tremors
- Valproate + DRAs/ Alcohol = Sedation, EPS
- Valproate + Anticoagulants (Aspirin/Warfarin) = augmentation of anticoagulant effect
- Valproate increases plasma conc of:
* Carbamazepine
* Diazepam
* Amitriptyline, Nortriptyline
* Phenobarbital
- Valproate decreases plasma conc of:
* Phenytoin
* Desipramine
- Plasma conc of Valproate increased by:
* Guanfacine
* Amitriptyline
* Fluoxetine
- Plasma conc of Valproate decreased by:
* Carbamazepine
(G) Laboratory Errors:
- False positive urine ketones
- falsely abnormal thyroid function test
- increase in serum fatty acids
(H) Therapeutic plasma concentration:
- For seizure control: 50-150 ug/mL (upto 200 ug/mL is well tolerated)
- For mental disorders: 50-125 ug/mL
- Most pt attain therapeutic plasma concentration on dosage between 1200- 1500 mg/day in divided doses.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Childhood Onset Schizophrenia- HY Facts
![]() Admin Mon Sep 12, 2011 11:05 am
Admin Mon Sep 12, 2011 11:05 am
- Occurs at age 12 years or younger and is often chronic and persistently debilitating
- According to the fourth edition of the DSM (DSM-IV), the criteria for childhood-onset schizophrenia and adult schizophrenia are synonymous, except for one potential modification for children (ie, in childhood-onset schizophrenia, the failure to meet expected social or academic milestones may be present, rather than deterioration in functioning).
- With the text revision of the DSM-IV (DSM-IV-TR), the criterion of social/occupational dysfunction in childhood or adolescent-onset schizophrenia can consist of a failure to achieve an expected level of interpersonal, academic, or occupational achievement.
- The prognosis for childhood-onset schizophrenia and adolescent-onset schizophrenia is worse than that observed in adult-onset schizophrenia.
- Patients with an onset before adolescence and those with an insidious onset appear to have a worse response to medication and a worse prognosis
- One half of these children have received previous diagnoses, including pervasive developmental disorders (PDDs), attention deficit hyperactivity disorder (ADHD), and internalizing disorders (eg, bipolar disorder, depression, anxiety disorders). In one study, psychotic symptoms appeared, on average, 2.5 years after the initial clinical presentation, and the diagnosis of schizophrenia was made a mean of 2 years after the onset of psychosis.
- Hallucinations (auditory more common than visual) are usually the presenting symptom and are reported by approximately 80% of children who receive the diagnosis of schizophrenia.
- Delusions are present in approximately 60% of patients.
- Ballageer et al found that bizarre behavior and negative symptoms were more common in individuals with adolescent-onset schizophrenia compared with those with onset during the adult years
- Compared with adults with schizophrenia, children with schizophrenia have catatonia less often
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Mon Sep 12, 2011 11:18 am
Admin Mon Sep 12, 2011 11:18 am
• Weight at baseline; 4, 8, and 12 weeks; and then quarterly
• Blood pressure at baseline, 12 weeks, and annually
• Fasting plasma glucose level at baseline, 12 weeks, and annually
• Fasting lipid profile at baseline, 12 weeks, and every 5 years
| Weight | Baseline | 4 Wk | 8 WK | 12 Wk | Quarterly |
| Blood Pressure | Baseline | 12 Wk | Annually | ||
| Fasting Blood Glucose | Baseline | 12 Wk | Annually | ||
| Fasting Lipid Profile | Baseline | 12 Wk | 5 yearly |
Similar recommendations regarding atypical antipsychotics are not yet available for children and adolescents, but careful monitoring of weight, blood pressure, and glucose and lipids levels seems warranted.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Mon Sep 12, 2011 12:13 pm
Admin Mon Sep 12, 2011 12:13 pm
Check out this link for details: http://bit.ly/nvJr5p
Last edited by Admin on Tue Sep 27, 2011 11:47 pm; edited 1 time in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Tue Sep 13, 2011 12:16 pm
Admin Tue Sep 13, 2011 12:16 pm
- Although the pathophysiology of NMS is complex—dopamine blockade likely plays a pivotal role in triggering the condition
- Agitation, dehydration, and exhaustion were found to be the most consistent systemic factors predisposing patients taking antipsychotics to NMS
Well-supported risk factors also include
* Use of high-potency antipsychotics,
* Prior episodes of NMS,
* Age <40,
* Male sex,
* Malnutrition,
* Organic brain syndromes, and
* Lithium use
- Can occur after the withdrawal of levodopa and similar dopaminergic agents during Parkinson’s disease treatment
- Management:
* Beyond supportive care, oral or IV benzodiazepines may relieve symptoms and speed recovery.
* Dopaminergic drugs, such as bromocriptine or amantadine, used alone or with other treatments, can reduce parkinsonism and disease duration and mortality.
* Dantrolene may be useful only for NMS patients who exhibit extreme temperature elevations, rigidity, and true hypermetabolism.
* ECT may be effective for NMS patients whose symptoms do not respond to supportive care and drug therapy or those with residual catatonic or parkinsonian symptoms
Last edited by Admin on Sat Aug 25, 2012 7:48 pm; edited 1 time in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Tue Sep 13, 2011 1:02 pm
Admin Tue Sep 13, 2011 1:02 pm
Susto:
Literally "fright", this generally falls into either natural or supernatural origin. Natural origins are cultural stressors, and are more likely to affect women than men. Supernatural origins may be thought to have been sent by a sorcerer, and may be triggered by witnessing supernatural phenomenon such as ghosts.
Symptoms include nervousness, anorexia, insomnia, listlessness, fatigue, despondency, muscle tics and diarrhea
Locura:
A chronic state of severe psychosis, attributed to multiple life stressors, inherited vulnerability, or a combination of both. Symptoms include agitation, incoherence, audio and visual hallucinations, inability to follow the rules of social interaction, unpredictability and possible violence.
Mal de ojo
The "evil eye". Children and infants are especially at risk. With adults, women are more likely to be affected. Symptoms include fitful sleep, crying inconsolably without apparent cause, diarrhea, vomiting and fever. It is most widespread in the Mediterranean and Near East cultures.
Mal de ojo is a Spanish phrase, and the idea is widespread in many Latino cultures. Typically, it is passed from someone who is strong to someone who is weaker, whether by status, wealth, or power, so the person at the greatest risk are those who have the lowest position, usually women, infants and young children. It is usually treated by traditional curanderos.
Sangue Dormido
"Sleeping blood," pain, numbness, tremor, paralysis, convulsions, stroke, blindness, heart attack, infection and miscarriage
Ataque de nervios:
Symptoms commonly include uncontrollable shouting, attacks of crying, trembling, heat in the chest rising into the head, and verbal and physical aggression. Some prominently feature dissociative episodes, seizure-like or fainting episodes, and suicidal gestures, while others lack those features entirely. A key feature is a sense of being out of control, and it is usually triggered by a stressful event within the family. It is commonly thought to be a result of a chronic build up of anger over time. People may not remember what they did during the ataque, and usually return to normal following the incident.
Bilis or cólera or muina
The cause of this disorder is seen to be a strongly expressed anger or rage, which disrupts the balance of both emotional and physical humors. Symptoms may include acute nervous tension, headache, trembling, screaming, stomach disturbances such as nausea, vomiting or diarrhea, and even loss of consciousness. Chronic fatigue may result from an acute episode.
The words bilis and cólera translate into bile and cholera, terms that are medical terms used to describe a bacterial disease (cholera) and the secretions of the intestines. This refers to the idea of humors, which has had a longstanding effect on medicine, and is based on the doctrine of Hippocrates. For instance, our term melancholy refers to the earth humor. A person who is raging may be described as spewing bile, and has a choleric humor. The concept of humor did not lose influence in the United States until the mid-20th century. It continues to be used in traditional medical systems and has an influence on the way we perceive our emotional states. Humors are about balance, and the disruption of balance leads to negative physical or emotional effects.
Mal puesto or brujeria
The conviction that illnesses are brought about by supernatural means, such as witchcraft, voodoo, or evil influence. Symptoms include anxiety, gastrointestinal complaints, and fear of being poisoned or killed.
Aire
Paralysis, twisted mouth, trembling, pimples and aching joints.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Tue Sep 13, 2011 7:34 pm
Admin Tue Sep 13, 2011 7:34 pm
Check the Next Post Below
Last edited by Admin on Tue Sep 13, 2011 7:37 pm; edited 1 time in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Tue Sep 13, 2011 7:35 pm
Admin Tue Sep 13, 2011 7:35 pm
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Thu Sep 15, 2011 11:35 am
Admin Thu Sep 15, 2011 11:35 am
This category should be used when there is a severe and pervasive impairment in the development of reciprocal social interaction associated with impairment in either verbal or nonverbal communication skills OR with the presence of stereotyped behavior, interests, and activities, BUT the criteria are not met for a specific Pervasive Developmental Disorder, Schizophrenia, Schizotypal Personality Disorder, or Avoidant Personality Disorder.
For example, this category includes "atypical autism"—presentations that do not meet the criteria for Autistic Disorder because of late age at onset, atypical symptomatology, or subthreshold symptomatology, or all of these.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Thu Sep 15, 2011 12:05 pm
Admin Thu Sep 15, 2011 12:05 pm
A.Either (1) or (2):
1. six (or more) of the following symptoms of inattention have persisted for at least 6 months to a degree that is maladaptive and inconsistent with developmental level:
Inattention
a. often fails to give close attention to details or makes careless mistakes in schoolwork, work, or other activities
b. often has difficulty sustaining attention in tasks or play activities
c. often does not seem to listen when spoken to directly
d. often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (not due to oppositional behavior or failure to understand instructions)
e. often has difficulty organizing tasks and activities
f. often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (such as schoolwork or homework)
g. often loses things necessary for tasks or activities (e.g., toys, school assignments, pencils, books, or tools)
h.is often easily distracted by extraneous stimuli
i. is often forgetful in daily activities
2. six (or more) of the following symptoms of hyperactivity-impulsivity have persisted for at least 6 months to a degree that is maladaptive and inconsistent with developmental level:
Hyperactivity
a. often fidgets with hands or feet or squirms in seat
b. often leaves seat in classroom or in other situations in which remaining seated is expected
c. often runs about or climbs excessively in situations in which it is inappropriate (in adolescents or adults, may be limited to subjective feelings of restlessness)
d. often has difficulty playing or engaging in leisure activities quietly
e. is often "on the go" or often acts as if "driven by a motor"
f. often talks excessively
Impulsivity
g. often blurts out answers before questions have been completed
h. often has difficulty awaiting turn
i. often interrupts or intrudes on others (e.g., butts into conversations or games)
B •Some hyperactive-impulsive or inattentive symptoms that caused impairment were present before age 7 years.
C •Some impairment from the symptoms is present in two or more settings (e.g., at school [or work] and at home).
D •There must be clear evidence of clinically significant impairment in social, academic, or occupational functioning.
E •The symptoms do not occur exclusively during the course of a Pervasive Developmental Disorder, Schizophrenia, or other Psychotic Disorder and are not better accounted for by another mental disorder (e.g., Mood Disorder, Anxiety Disorder, Dissociative Disorder, or a Personality Disorder).
Code based on type:
314.01 Attention-Deficit/Hyperactivity Disorder, Combined Type: if both Criteria A1 and A2 are met for the past 6 months
314.00 Attention-Deficit/Hyperactivity Disorder, Predominantly Inattentive Type: if Criterion A1 is met but Criterion A2 is not met for the past 6 months
314.01 Attention-Deficit/Hyperactivity Disorder, Predominantly Hyperactive-Impulsive Type: if Criterion A2 is met but Criterion A1 is not met for the past 6 months
Coding note: For individuals (especially adolescents and adults) who currently have symptoms that no longer meet full criteria, "In Partial Remission" should be specified.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Fri Sep 16, 2011 1:13 pm
Admin Fri Sep 16, 2011 1:13 pm
Presence of both criteria (A) & (B)
A. A strong and persistent cross-gender identification (not merely a desire for any perceived cultural advantages of being the other sex).
In children, the disturbance is manifested by four (or more) of the following:
- repeatedly stated desire to be, or insistence that he or she is, the other sex
- in boys, preference for cross-dressing or simulating female attire; in girls, insistence on wearing only stereotypical masculine clothing
- strong and persistent preferences for cross-sex roles in make-believe play or persistent fantasies of being the other sex
- intense desire to participate in the stereotypical games and pastimes of the other sex
- strong preference for playmates of the other sex
In adolescents and adults, the disturbance is manifested by symptoms such as a
- stated desire to be the other sex,
- frequent passing as the other sex,
- desire to live or be treated as the other sex, or
- the conviction that he or she has the typical feelings and reactions of the other sex.
B. Persistent discomfort with his or her sex or sense of inappropriateness in the gender role of that sex.
In children, the disturbance is manifested by any of the following:
- in boys, assertion that his penis or testes are disgusting or will disappear or assertion that it would be better not to have a penis, or aversion toward rough-and-tumble play and rejection of male stereotypical toys, games, and activities;
- in girls, rejection of urinating in a sitting position, assertion that she has or will grow a penis, or assertion that she does not want to grow breasts or menstruate, or marked aversion toward normative feminine clothing.
In adolescents and adults, the disturbance is manifested by symptoms such as
- preoccupation with getting rid of primary and secondary sex characteristics (e.g., request for hormones, surgery, or other procedures to physically alter sexual characteristics to simulate the other sex) or
- belief that he or she was born the wrong sex.
C. The disturbance is not concurrent with a physical intersex condition.
D. The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Code based on current age:
302.6 Gender Identity Disorder in Children
302.85 Gender Identity Disorder in Adolescents or Adults
Specify if (for sexually mature individuals):
- Sexually Attracted to Males
- Sexually Attracted to Females
- Sexually Attracted to Both
- Sexually Attracted to Neither
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Fri Sep 16, 2011 2:08 pm
Admin Fri Sep 16, 2011 2:08 pm
Preconscious or Subconscious:
- This is the part of us that we can access if prompted, but is not in our active conscious. Its right below the surface, but still buried somewhat unless we search for it.
- Information such as our telephone number, some childhood memories, or the name of your best childhood friend is stored in the preconscious.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sat Sep 17, 2011 1:50 pm
Admin Sat Sep 17, 2011 1:50 pm
Toxoplasmosis: Ring enhancing lesion on MRI; Gold standard for diagnosis: PCR, Toxo Ab
CNS Lymphoma: Mass lesion on MRI
Cryptococcal Meningitis: Fungal infection of CNS, inc pressures, meningeal signs; Tt: Ampho B
Progressive Multifocal Leuckoencephalopathy: JC virus, multifocal demyelination; Sx: Clumsiness, progressive weakness, abnormalities in vision, speech & personality; Dx: CSF & Imaging
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sat Sep 17, 2011 2:53 pm
Admin Sat Sep 17, 2011 2:53 pm
Shuffling Gait-
Cause: Parkinson Disease
Rapid shuffling steps and a forward-flexed posture when walking
Ataxic gait:
Cause:Alcohol Cerebellar Degeneration :
Broad based gait
Neuropathic Gait (Steppage gait):
Cause: Damage to the deep peroneal nerve
Dragging foot and high steps while walking.
Choreiform Gait:
Associated with involuntary movements (chorea) superimposed on gait.
Trendelenburg gait/ Myopathic Gait/ Waddling gait
Cause: Myopathies of Pelvic girdle, lesion of superior gluteal nerve, L5 radiculopathy and after poliomyelitis
Hyperlordotic posture and swing toward weight bearing leg while walking.
Scissor gait/ Diplegic Gait
Cause: spastic cerebral palsy, upper motor neuron lesion
Hypertonia in the legs, hips and pelvis means these areas become flexed, to various degrees, giving the appearance of crouching, while tight adductors produce extreme adduction, presented by knees and thighs hitting, or sometimes even crossing, in a scissors-like movement while the opposing muscles, the abductors, become comparatively weak from lack of use.
Conversion Disorder: Astasia-Abasia Gait- refers to the inability to either stand or walk in a normal manner. Patients exhibit an unusual and dramatic gait disturbance, lurching wildly in various directions and falling only when a nearby physician, family member, or soft object will catch them.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sat Sep 17, 2011 3:22 pm
Admin Sat Sep 17, 2011 3:22 pm
Post Herpetic Neuralgia, which occurs after shingles (VGV), may have similar symptoms to Trigeminal Neuralgia if Trigeminal Nerve is affected.
Differentiate by presence of associated vescicles, and unremitting pain (not lasting seconds) following the dermatomes
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sat Sep 17, 2011 5:28 pm
Admin Sat Sep 17, 2011 5:28 pm
Details here: http://bit.ly/pRGG18
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sat Sep 17, 2011 7:28 pm
Admin Sat Sep 17, 2011 7:28 pm
| Nerve Root | L4 | L5 | S1 |
| Motor Weakness | Extension of Quadriceps | Dorsiflexion of greater toe & foot | Plantar flexion of greater toe & foot |
| Screening Exam | Squat & Rise | Heel walking | Toe walking |
| Reflexes | Knee jerk diminished | None reliable | Ankle jerk diminished |
Sciatic Nerve involvement: more diffuse (L4-S3 involved)
Peroneal N (branch of Sciatic N): Loss of dorsiflexion (Foot drop)
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sun Sep 18, 2011 6:19 pm
Admin Sun Sep 18, 2011 6:19 pm
| Classic Conditioning | Operant Conditioning |
| Classical conditioning involves pairing a previously neutral stimulus (such as the sound of a bell) with an unconditioned stimulus (the taste of food). This unconditioned stimulus naturally and automatically triggers salivating as a response to the food, which is known as the unconditioned response. After associating the neutral stimulus and the unconditioned stimulus, the sound of the bell alone will start to evoke salivating as a response. The sound of the bell is now known as the conditioned stimulus and salivating in response to the bell is known as the conditioned response. (check pic below) | Operant conditioning focuses on using either reinforcement or punishment to increase or decrease a behavior. Through this process, an association is formed between the behavior and the consequences for that behavior. For example, imagine that a trainer is trying to teach a dog to fetch a ball. When the dog successful chases and picks up the ball, the dog receives praise as a reward. When the animal fails to retrieve the ball, the trainer withholds the praise. Eventually, the dog forms an association between his behavior of fetching the ball and receiving the desired reward. |
| Involves placing a neutral signal before a reflex | Involves applying reinforcement or punishment after a behavior |
| Focuses on involuntary, automatic behaviors | Focuses on strengthening or weakening voluntary behaviors |
One of the simplest ways to remember the differences between classical and operant conditioning is to focus on whether the behavior is involuntary or voluntary. Classical conditioning involves making an association between an involuntary response and a stimulus, while operant conditioning is about making an association between a voluntary behavior and a consequence.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sun Sep 18, 2011 7:57 pm
Admin Sun Sep 18, 2011 7:57 pm

Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Page 2 of 4 • 1, 2, 3, 4 ![]()
» Supportive Psychotherapy- High Yield Facts
» Personality Disorders (10 High Yield Facts)
» prite exam
» PRITE Oriented Topics
FORUM FOR PSYCHIATRY RESIDENTS :: Psychiatry :: Psychiatry-Neurology-Psychology discussion :: Psychiatry In Depth
» L-Methylfolate: Who Will benefit
» Vitamins & Supplements in Clinical Practice.
» Imaging Biomarkers for Outcomes in Mild TBI
» Q.5 Clozapine Neutopenia
» Treating Disorders!
» Cortical Abnormalities in Adults & Adolescents with MDD
» Efficacy of Antipsychotics in Pediatric Acute Mania
» Obsessive Compulsive Disorder in Adults: Which Treatment is Better?