

Search
Statistics
We have 222 registered usersThe newest registered user is raheelmemon
Our users have posted a total of 1140 messages in 613 subjects
If you are seeing this, you have attempted to link to the UpToDate widget but are experiencing a problem. Please visit UpToDate for more information.

LITHIUM- Question Series (Check Your Basics)
4 posters
FORUM FOR PSYCHIATRY RESIDENTS :: Psychiatry :: Psychiatry-Neurology-Psychology discussion :: Psycho-Pharmacology
Page 1 of 1

LITHIUM- Question Series (Check Your Basics)
![]() Admin Thu Dec 15, 2011 2:00 am
Admin Thu Dec 15, 2011 2:00 am
LITHIUM- Question Series
This thread is dedicated to questions related to LITHIUM:
I would encourage all members on this Forum, Facebook & Twitter to participate.
This thread will cover all clinical and PRITE related facts on LITHIUM.
Thanks
Admin
**Answers with Explanation will be posted after member's have submitted there answers **


This thread is dedicated to questions related to LITHIUM:
I would encourage all members on this Forum, Facebook & Twitter to participate.
This thread will cover all clinical and PRITE related facts on LITHIUM.
Thanks
Admin
**Answers with Explanation will be posted after member's have submitted there answers **
Last edited by Admin on Mon Oct 15, 2012 9:03 pm; edited 3 times in total

Admin- Admin

- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -

Re: LITHIUM- Question Series (Check Your Basics)
![]() Admin Thu Dec 15, 2011 2:05 am
Admin Thu Dec 15, 2011 2:05 am

Which of the following statement is FALSE regarding LITHIUM:
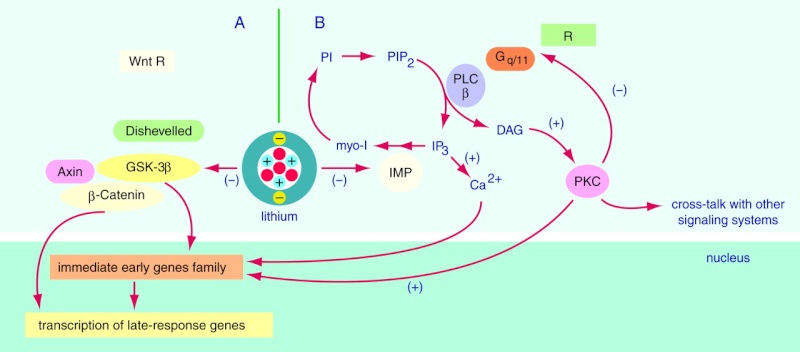
(a) Lithium directly inhibits Glycogen Synthase Kinase 3B & Inositol monophosphate Phosphatase
(b) Lithium use in bipolar disorder can result in increase cortical gray matter & Hippocampal Volume.
(c) It takes at least 4-5 days for serum lithium levels to reach steady state after the dose is changed
(d) Food alters the Lithium absorption.
(e) Once daily lithium level of 1.0 meq/L is expected to drop to a level of 0.8 meq/L if the patient switches to a divided dose regimen
Last edited by Admin on Sun Jan 15, 2012 10:26 pm; edited 2 times in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: LITHIUM- Question Series (Check Your Basics)
![]() Admin Thu Dec 15, 2011 2:23 am
Admin Thu Dec 15, 2011 2:23 am

Which of the following condition is not a contraindication for Lithium use?
(a) Dehydration
(b) Psoriasis
(c) Significant renal impairment
(d) Sodium Depletion
(e) Significant cardiovascular disease
(f) All are contraindication for Lithium use
(g) None of them are contraindication for Lithium use
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: LITHIUM- Question Series (Check Your Basics)
![]() Admin Thu Dec 15, 2011 3:09 am
Admin Thu Dec 15, 2011 3:09 am

Select the FALSE statement regarding "Lithium levels"
(a) Levels ≥ 2.5 mEq/L constitute a medical emergency, even in patients who appear relatively asymptomatic.
(b) Thiazide diuretics increases, and potassium sparing diuretics decreases Lithium levels
(c) Concomitant use of Metronidazole can lower Lithium levels
(d) Thyroid Function Tests should be monitored every 2-3 months during the first six months of Lithium therapy, and every 6 to 12 months thereafter
Last edited by Admin on Sun Jan 15, 2012 10:31 pm; edited 1 time in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: LITHIUM- Question Series (Check Your Basics)
![]() Admin Fri Dec 16, 2011 3:07 am
Admin Fri Dec 16, 2011 3:07 am

Which of the following statement is incorrect regarding "Lithium Side Effects"?
(a) Clinicians should consult a nephrologist and discontinue lithium when the serum creatinine approaches or exceeds 1.6 mg/dL.
(b) Neither pretreatment hypothyroidism nor lithium-induced hypothyroidism is a contraindication to lithium therapy.
(c) ECG is recommended in patients > 40 yr age
(d) All the statements are correct
(e) All the statements are wrong
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: LITHIUM- Question Series (Check Your Basics)
![]() drrodrick Tue Dec 27, 2011 5:08 am
drrodrick Tue Dec 27, 2011 5:08 am
This is really awesome post. I really like it. I have no words for it. Thanks for sharing.
USMLE
USMLE
drrodrick- Posts : 3
Points : 7
Reputation : 0
Join date : 2011-12-19
Re: LITHIUM- Question Series (Check Your Basics)
![]() P450 Sun Jan 22, 2012 7:25 pm
P450 Sun Jan 22, 2012 7:25 pm
I'll take a crack at these:
Q1: Which of the following statement is FALSE regarding LITHIUM:
(a) Lithium directly inhibits Glycogen Synthase Kinase 3B & Inositol monophosphate Phosphatase
(b) Lithium use in bipolar disorder can result in increase cortical gray matter & Hippocampal Volume.
(c) It takes at least 4-5 days for serum lithium levels to reach steady state after the dose is changed
(d) Food alters the Lithium absorption.
(e) Once daily lithium level of 1.0 meq/L is expected to drop to a level of 0.8 meq/L if the patient switches to a divided dose regimen
B: False --> I don't know of any data showing increase in brain volume
Q2: Which of the following condition is not a contraindication for Lithium use?
(a) Dehydration
(b) Psoriasis
(c) Significant renal impairment
(d) Sodium Depletion
(e) Significant cardiovascular disease
(f) All are contraindication for Lithium use
(g) None of them are contraindication for Lithium use
G: None --> Maybe a relative contraindication for a couple of these.
Q3: Select the FALSE statement regarding "Lithium levels"
(a) Levels ≥ 2.5 mEq/L constitute a medical emergency, even in patients who appear relatively asymptomatic.
(b) Thiazide diuretics increases, and potassium sparing diuretics decreases Lithium levels
(c) Concomitant use of Metronidazole can lower Lithium levels
(d) Thyroid Function Tests should be monitored every 2-3 months during the first six months of Lithium therapy, and every 6 to 12 months thereafter
C: Don't recall metronidazole having any effect on GFR or absorption.
Q4:Which of the following statement is incorrect regarding "Lithium Side Effects"?
(a) Clinicians should consult a nephrologist and discontinue lithium when the serum creatinine approaches or exceeds 1.6 mg/dL.
(b) Neither pretreatment hypothyroidism nor lithium-induced hypothyroidism is a contraindication to lithium therapy.
(c) ECG is recommended in patients > 40 yr age
(d) All the statements are correct
(e) All the statements are wrong
A: You can simply lower the dose of lithium and of course monitor Li levels. The increase in Cr may have nothing to do with the lithium.
Q1: Which of the following statement is FALSE regarding LITHIUM:
(a) Lithium directly inhibits Glycogen Synthase Kinase 3B & Inositol monophosphate Phosphatase
(b) Lithium use in bipolar disorder can result in increase cortical gray matter & Hippocampal Volume.
(c) It takes at least 4-5 days for serum lithium levels to reach steady state after the dose is changed
(d) Food alters the Lithium absorption.
(e) Once daily lithium level of 1.0 meq/L is expected to drop to a level of 0.8 meq/L if the patient switches to a divided dose regimen
B: False --> I don't know of any data showing increase in brain volume
Q2: Which of the following condition is not a contraindication for Lithium use?
(a) Dehydration
(b) Psoriasis
(c) Significant renal impairment
(d) Sodium Depletion
(e) Significant cardiovascular disease
(f) All are contraindication for Lithium use
(g) None of them are contraindication for Lithium use
G: None --> Maybe a relative contraindication for a couple of these.
Q3: Select the FALSE statement regarding "Lithium levels"
(a) Levels ≥ 2.5 mEq/L constitute a medical emergency, even in patients who appear relatively asymptomatic.
(b) Thiazide diuretics increases, and potassium sparing diuretics decreases Lithium levels
(c) Concomitant use of Metronidazole can lower Lithium levels
(d) Thyroid Function Tests should be monitored every 2-3 months during the first six months of Lithium therapy, and every 6 to 12 months thereafter
C: Don't recall metronidazole having any effect on GFR or absorption.
Q4:Which of the following statement is incorrect regarding "Lithium Side Effects"?
(a) Clinicians should consult a nephrologist and discontinue lithium when the serum creatinine approaches or exceeds 1.6 mg/dL.
(b) Neither pretreatment hypothyroidism nor lithium-induced hypothyroidism is a contraindication to lithium therapy.
(c) ECG is recommended in patients > 40 yr age
(d) All the statements are correct
(e) All the statements are wrong
A: You can simply lower the dose of lithium and of course monitor Li levels. The increase in Cr may have nothing to do with the lithium.
P450- Moderator

- Posts : 34
Points : 34
Reputation : 0
Join date : 2012-01-15
Re: LITHIUM- Question Series (Check Your Basics)
![]() Admin Sun Jan 22, 2012 7:58 pm
Admin Sun Jan 22, 2012 7:58 pm
Admin wrote:
Which of the following statement is FALSE regarding LITHIUM:
(a) Lithium directly inhibits Glycogen Synthase Kinase 3B & Inositol monophosphate Phosphatase
(b) Lithium use in bipolar disorder can result in increase cortical gray matter & Hippocampal Volume.
(c) It takes at least 4-5 days for serum lithium levels to reach steady state after the dose is changed
(d) Food alters the Lithium absorption.
(e) Once daily lithium level of 1.0 meq/L is expected to drop to a level of 0.8 meq/L if the patient switches to a divided dose regimen
Answer: C.
- Lithium is rapidly absorbed through the gastrointestinal tract; food does not alter lithium absorption.
(Source: UpToDate)
- Lithium directly inhibits Glycogen Synthase Kinase 3B & Inositol monophosphate Phosphatase
(Source: http://ajp.psychiatryonline.org/article.aspx?articleID=173733)
- Lithium also appears to increase neurogenesis and neuroprotective factors, and in patients with bipolar disorder, increase cortical gray matter and hippocampal volume.
(Source: Molecular actions and therapeutic potential of lithium in preclinical and clinical studies of CNS disorders.Pharmacol Ther. 2010;128(2):281.)
(Source: In search of the Holy Grail for the treatment of neurodegenerative disorders: has a simple cation been overlooked? Biol Psychiatry. 2007;62(1):4.)
- When lithium is taken once per day, serum levels are approximately 25 percent higher compared with levels when lithium is taken two or three times per day, due to changes in renal excretion. Therefore, a once daily lithium level of 1.0 meq/L is expected to drop to a level of 0.8 meq/L if the patient switches to a divided dose regimen. Virtually all studies examining optimal lithium levels have used divided dose regimens.
(Source: UpToDate)
Admin wrote:
Which of the following condition is not a contraindication for Lithium use?
(a) Dehydration
(b) Psoriasis
(c) Significant renal impairment
(d) Sodium Depletion
(e) Significant cardiovascular disease
(f) All are contraindication for Lithium use
(g) None of them are contraindication for Lithium use
Answer: F. All are contraindication for Lithium use
Contraindications —
- Significant renal impairment
- Sodium depletion
- Dehydration
- Significant cardiovascular disease (lithium can rarely cause sinus node dysfunction- eg, sinus bradycardia and sinoatrial block; atrioventricular node dissociation with atrioventricular block and junctional rhythms; and ventricular premature beats).
- Psoriasis, which lithium exacerbates, is a relative contraindication.
(Source: UpToDate)
Admin wrote:
Select the FALSE statement regarding "Lithium levels"
(a) Levels ≥ 2.5 mEq/L constitute a medical emergency, even in patients who appear relatively asymptomatic.
(b) Thiazide diuretics increases, and potassium sparing diuretics decreases Lithium levels
(c) Concomitant use of Metronidazole can lower Lithium levels
(d) Thyroid Function Tests should be monitored every 2-3 months during the first six months of Lithium therapy, and every 6 to 12 months thereafter
Answer: C.
- Concomitant use of Metronidazole can INCREASE Lithium levels
- Lithium toxicity is a clinical diagnosis that is confirmed by serum lithium levels.
Relatively mild toxicity usually does not occur until serum lithium reaches a level of 1.5 mEq/L (1.5 mmol/L).
Levels ≥ 2.5 mEq/L (2.5 mmol/L) constitute a medical emergency, even in patients who appear relatively asymptomatic.
The likelihood of lithium intoxication is increased when lithium excretion is impaired. This most commonly occurs with:
> Underlying renal insufficiency
> Effective volume depletion
> Elderly patients (low glomerular filtration rate)
(Source: UpToDate)
- Medications that Increases lithium level
> Thiazide diuretics
> Nonsteroidal antiinflammatory drugs (NSAIDS) except aspirin
> Angiotensin converting enzyme (ACE) inhibitors
> Antibiotics tetracyclines and metronidazole
- Medications that Decreases lithium level
> Potassium-sparing diuretics
> Theophylline
(Source: UpToDate)
Admin wrote:
Which of the following statement is incorrect regarding "Lithium Side Effects"?
(a) Clinicians should consult a nephrologist and discontinue lithium when the serum creatinine approaches or exceeds 1.6 mg/dL.
(b) Neither pretreatment hypothyroidism nor lithium-induced hypothyroidism is a contraindication to lithium therapy.
(c) ECG is recommended in patients > 40 yr age
(d) All the statements are correct
(e) All the statements are wrong
Even I thought answer is A.
But correct answer= (d) All the statements are correct
- Lithium has a deleterious effect on renal tubular function. Initially, lithium reduces the ability of the kidney to concentrate urine, leading to dilute urine and polyuria (nephrogenic diabetes insipidus). Over months and years, this functional deficit becomes structural. Biopsy specimens from patients chronically treated with lithium show interstitial fibrosis that is consistent with chronic interstitial nephritis in more severe cases. If patients drink enough when they are thirsty, this is not dangerous. However, this process can lead to increased serum creatinine and, rarely, to progressive renal failure. Thus, monitoring renal function by serial serum creatinine is an essential part of ongoing lithium therapy. Clinicians should consult a nephrologist and discontinue lithium when the serum creatinine approaches or exceeds 1.6 mg/dL (140 mmol/L). The most important risk factor for renal damage from lithium is repeated episodes of lithium intoxication.
(Source: UpToDate)
- Lithium interferes with function of the thyroid gland and can cause goiter, hypothyroidism, chronic autoimmune thyroiditis, and possibly hyperthyroidism. Neither pretreatment hypothyroidism (presumably treated adequately with T4) nor lithium-induced hypothyroidism is a contraindication to lithium therapy. Reasonable recommendations are to monitor serum TSH and if it rises much above the upper value of normal, to start T4 while continuing the lithium.
(Source: UpToDate)
Thanks again for participating P450.
Regards
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: LITHIUM- Question Series (Check Your Basics)
![]() P450 Sun Jan 22, 2012 9:05 pm
P450 Sun Jan 22, 2012 9:05 pm
Good to know! Thanks Harvinder.
P450- Moderator
- Posts : 34
Points : 34
Reputation : 0
Join date : 2012-01-15
Re: LITHIUM- Question Series (Check Your Basics)
![]() Admin Sun Jan 22, 2012 9:14 pm
Admin Sun Jan 22, 2012 9:14 pm
Thanks buddy 
Do try rest of the questions from Psychopharmacology thread:
https://psychiatry.forumotion.com/t197-psychopharmacology-discussion-thread
I like this discussion.
Do try rest of the questions from Psychopharmacology thread:
https://psychiatry.forumotion.com/t197-psychopharmacology-discussion-thread
I like this discussion.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: LITHIUM- Question Series (Check Your Basics)
![]() adisuper Mon Oct 15, 2012 12:56 pm
adisuper Mon Oct 15, 2012 12:56 pm
in question 3 option b it's written that potassium sparing diuretics decrease lithium levels but as per ctp table 31.19-4 they could possibly increase lithium level by causing lithium retention. Which one is correct...
adisuper- Posts : 28
Points : 32
Reputation : 0
Join date : 2012-06-04
Re: LITHIUM- Question Series (Check Your Basics)
![]() Admin Mon Oct 15, 2012 9:01 pm
Admin Mon Oct 15, 2012 9:01 pm
Hi Adisuper.
This is confusing for me too.
Check the following information from UpToDate:
Source used by UpToDate:
Labbate, LA, Fava, M, Rosenbaum, JF, et al. Drugs for treatment of bipolar disorders. In: Handbook of Psychiatric Drug Therapy, 6th ed, Lippincott Williams & Wilkins, Philadelphia 2010. p.110.
Can anyone Explain the mechanism of interaction between Lithium and Diuretics.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: LITHIUM- Question Series (Check Your Basics)
![]() adisuper Tue Oct 16, 2012 9:24 am
adisuper Tue Oct 16, 2012 9:24 am
Documentation Level:
Limited - Few reports of this interaction exist. These few reports usually consist of limited case reports where clinically sound justification of the interaction is found.
Probable Mechanism:
Generally, diuretics may reduce lithium clearance, resulting in increased lithium levels and possible toxicity. Spironolactone has been reported to increase lithium levels in one report
This is as per MIMS website which quotes following references
Reference:
MedicinesComplete: Sweetman S (ed). Spironolactone: Martindale: The Complete Drug Reference. RPS Publishing, London, UK, Available from URL: http://www.medicinescomplete.com/mc [Accessed on 22/07/2010]
MedicinesComplete: Baxter K (ed). Lithium + Diuretics; Potassium-sparing: Stockleys Drug Interactions. RPS Publishing, London, UK, Available from URL: http://www.medicinescomplete.com/mc [Accessed on 22/07/2010]
Loop diuretics e.g. Furosemide (frusemide), bumetanide, and Potassium Sparing Diuretics e.g.
amiloride, spironolatone are safer than thiazide diuretics but not without risks of Lithium toxicity
References
BNF No 48 September 2004
Psychotropic Drug Directory 2003/04. Stephen Bazire.
Limited - Few reports of this interaction exist. These few reports usually consist of limited case reports where clinically sound justification of the interaction is found.
Probable Mechanism:
Generally, diuretics may reduce lithium clearance, resulting in increased lithium levels and possible toxicity. Spironolactone has been reported to increase lithium levels in one report
This is as per MIMS website which quotes following references
Reference:
MedicinesComplete: Sweetman S (ed). Spironolactone: Martindale: The Complete Drug Reference. RPS Publishing, London, UK, Available from URL: http://www.medicinescomplete.com/mc [Accessed on 22/07/2010]
MedicinesComplete: Baxter K (ed). Lithium + Diuretics; Potassium-sparing: Stockleys Drug Interactions. RPS Publishing, London, UK, Available from URL: http://www.medicinescomplete.com/mc [Accessed on 22/07/2010]
Loop diuretics e.g. Furosemide (frusemide), bumetanide, and Potassium Sparing Diuretics e.g.
amiloride, spironolatone are safer than thiazide diuretics but not without risks of Lithium toxicity
References
BNF No 48 September 2004
Psychotropic Drug Directory 2003/04. Stephen Bazire.
adisuper- Posts : 28
Points : 32
Reputation : 0
Join date : 2012-06-04
» Bupropion- Check Your Basics
» Check your Basics: Benzodiazepines
» Serotonin Pathway: Check Your Basics
» Valproate (Depakote): Check Your Basics
» Psychopharmacology Weekly Question Series- Don't Miss Out !!
» Check your Basics: Benzodiazepines
» Serotonin Pathway: Check Your Basics
» Valproate (Depakote): Check Your Basics
» Psychopharmacology Weekly Question Series- Don't Miss Out !!
FORUM FOR PSYCHIATRY RESIDENTS :: Psychiatry :: Psychiatry-Neurology-Psychology discussion :: Psycho-Pharmacology
Page 1 of 1
Permissions in this forum:
You cannot reply to topics in this forum
» L-Methylfolate: Who Will benefit
» Vitamins & Supplements in Clinical Practice.
» Imaging Biomarkers for Outcomes in Mild TBI
» Q.5 Clozapine Neutopenia
» Treating Disorders!
» Cortical Abnormalities in Adults & Adolescents with MDD
» Efficacy of Antipsychotics in Pediatric Acute Mania
» Obsessive Compulsive Disorder in Adults: Which Treatment is Better?