

The newest registered user is raheelmemon
Our users have posted a total of 1140 messages in 613 subjects

PRITE High Yield Topic Discussion Thread
FORUM FOR PSYCHIATRY RESIDENTS :: Psychiatry :: Psychiatry-Neurology-Psychology discussion :: Psychiatry In Depth
Page 1 of 4 • 1, 2, 3, 4 ![]()

PRITE High Yield Topic Discussion Thread
![]() Admin Sun Sep 04, 2011 9:45 pm
Admin Sun Sep 04, 2011 9:45 pm
This thread is dedicated to PRITE (Psychiatry Resident-In-Training Examination) Preparation.
Please contribute important high yield topics and notes here.

INDEX:
Page 1:
• Typical Antipsychotics
• Borderline Personality Disorder
• Schizophrenia
• Dopaminergic Pathway Functions & Effect of Antipsychotics
• Sigmund Freud’s Structural Model- The id, ego, and superego
• Major depression with Atypical features
• Akathisia treatment
• Rabbit Syndrome
• Risperidone vs Clozapine
Page 2:
• Cluster A Personality disorder- differential diagnosis
• Cluster B Personality disorder- differential diagnosis
• Cluster C Personality disorder- differential diagnosis
• Personality disorder in toto (HY Facts)
• Frontotemporal dementia Vs Alzheimer’s dementia
• Autoreceptors Vs Heteroreceptors
• Visual Pathway And Associated Visual Defects
• Myasthenia Gravis
• Jean Piaget's Cognitive Development Stages
• Normal Aging- Facts
• Erikson's Stages of Psychosocial Development
• Cognitive Theory for depression Management
Page 3:
• Interpersonal Therapy (IPT)
• Valproate
• Childhood Onset Schizophrenia
• Recommendations for monitoring adults on atypical antipsychotics
• Pediatric Depression- Which SSRI is Superior
• Neuroleptic Malignant Syndrome
• Hispanic culture-bound syndromes
• Elevated Clozapine Levels
• Pervasive Developmental Disorder Not Otherwise Specified (Including Atypical Autism)
• Diagnostic criteria for Attention-Deficit/Hyperactivity Disorder
• Diagnostic criteria for Gender Identity Disorder
• Freud's Topographical Model
• HIV Dementia/Toxoplasmosis/CNS Lymphoma/Cryptococcal Meningitis/PML
• Gait Abnormalities
Page 4:
• Trigeminal neuralgia Vs Post Herpetic Neuralgia
• Carbon Monoxide Toxicity: Brain MRI Findings
• Lumbar & Sacral Nerve Root Compromise
• Classic Conditioning Vs Operant Conditioning
• Observational Study Design: Case control Vs Cohort
• Alexia/Apraxia/Agnosia/Akinesia/Aphasia
• Adjustment Disorders Vs Acute Stress Disorder
• SNRIs: Venlafaxine Vs Duloxetine
• DSM IV Criteria for Manic Episode
• Bipolar Disorder: 15 Minutes CORE Psychiatric Evaluation- 4 Decision Points
• Bipolar Depression Vs Unipolar Depression
• Difference Between Classical Conditioning & Extinction
• "Neurology" Questions/HY Facts for PRITE (Post 1 & 2)
Page 5:
• Catatonia
• CVA
• "Delirium" & "Dementia"
• Seizure
• Obsessive-compulsive disorders
• Role of Ziprasidone in combination therapy for Bipolar maintenance
• Recognition of GAD in Primary Care Setting
• Social Anxiety Disorder
• Panic Disorder
• ADHD (Recent Facts)
• Basics of Nor-Epinephrine, Dopamine & Seretonin Neurons.
• Hyperprolactinaemia With Antipsychotics
• Idiopathic Parkinson Ds Vs Other Parkinsonian Syndrome
• Pathophysiology of Neuroleptic Malignant Syndrome (NMS)
Page 6:
• Treatment of Juvenile Myoclonic Epilepsy
• Borderline Personality Disorder- What Questions to Ask?
• Transient Global Amnesia- Facts.
• Effective Dose for Antipsychotics- ED50 & Near-Maximal ED
• Fatal Familial Insomnia
• Medications for Alcohol Dependence
• Serotonin Toxicity- Diagnostic Criteria
• Alexithymia
• AACAP Practice Parameters for Bipolar Disorder in Children
• Progressive Supranuclear Palsy Vs Parkinson's disease
• Treatment of Depression with Atypical Features
• Types of Aphasia
• The Social Learning Theory of Julian B. Rotter
***** Updated Daily *****
Regards
Administrator
Last edited by Admin on Sun Nov 24, 2013 7:29 pm; edited 67 times in total

Admin- Admin

- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -

Re: PRITE High Yield Topic Discussion Thread
![]() Admin Sun Sep 04, 2011 11:54 pm
Admin Sun Sep 04, 2011 11:54 pm
1 • Following a first episode of psychosis: patient maintained on medications for 1-2 years.
• Following a second episode of psychosis: patient maintained for 2-5 years.
• Following multiple episodes: patient maintained on lifelong treatment.
2 • In cases of Phencyclidine intoxications: Benzodiazepines should be used instead of DRAs.
Reason: Anticholinergic effect of DRAs
3 • In patients experiencing hallucinations or delusions result of alcohol withdrawal: DRAs may increase the risk of seizure.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() psychinmymind Mon Sep 05, 2011 2:56 pm
psychinmymind Mon Sep 05, 2011 2:56 pm
Splitting, denial, projection, projective identification, acting out, idealization, and devaluation.
psychinmymind- Moderator

- Posts : 24
Points : 44
Reputation : 3
Join date : 2011-04-14
Location : Arizona
Re: PRITE High Yield Topic Discussion Thread
![]() psychinmymind Mon Sep 05, 2011 2:58 pm
psychinmymind Mon Sep 05, 2011 2:58 pm
of trauma is the amygdala which is consistently reduced in volume. ALso, there is associated hyperactivity of the amygdala. The hypothalamic pituitary adrenal axis has also been shown to be hyperactive in these individuals.
psychinmymind- Moderator
- Posts : 24
Points : 44
Reputation : 3
Join date : 2011-04-14
Location : Arizona
Re: PRITE High Yield Topic Discussion Thread
![]() psychinmymind Mon Sep 05, 2011 2:59 pm
psychinmymind Mon Sep 05, 2011 2:59 pm
Reason: Anticholinergic effect of DRAs
psychinmymind- Moderator
- Posts : 24
Points : 44
Reputation : 3
Join date : 2011-04-14
Location : Arizona
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Mon Sep 05, 2011 7:53 pm
Admin Mon Sep 05, 2011 7:53 pm
psychinmymind wrote:Admin, Could you please explain more on 2 • In cases of Phencyclidine intoxications: Benzodiazepines should be used instead of DRAs.
Reason: Anticholinergic effect of DRAs
Explanation is as follows:
At high doses of Phencyclidine (PCP) use- PCP have anticholinergic action. Hence neuroleptics with potent intrinsic anticholinergic property should be avoided. As a precautionary measure- BZD should be used first followed by DRAs, but there is no convincing evidence that either of them is clinically superior.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Mon Sep 05, 2011 8:06 pm
Admin Mon Sep 05, 2011 8:06 pm
* First Rank symptoms of Kurt Schneider indicates poor prognosis.
First rank symptoms include:
- Audible thoughts
- Voice arguing or discussing or both
- Voice commenting
- Somatic passivity experience (e.g., control of pt body by influence of other)
- Thought withdrawal & other experiences of influenced thought
- Thought broadcasting
- Delusional perceptions
- All other experiences invloving volition made affect, and made impulses.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Mon Sep 05, 2011 8:29 pm
Admin Mon Sep 05, 2011 8:29 pm
Q- What is the reason for "Auditory Hallucinations" in Schizophrenics
Schizophrenic pt exhibits an inability to filter out irrelevant sounds & are extremely sensitive to background noise. The flooding of sounds that results make concentration difficult & may be a factor in production of auditory hallucinations.
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Mon Sep 05, 2011 8:57 pm
Admin Mon Sep 05, 2011 8:57 pm
| Dopamine Track | Pathway | Function | Antipsychotic Drug Effect |
| Nigrostriatal | substantia nigra in the midbrain to the caudate nucleus in the basal ganglia | Extrapyramidal System | Movement disorders |
| Mesolimbic | midbrain to limbic system | Arousal, Memory, Stimulus processing, Motivation | Relief of Psychosis |
| Mesocortical | midbrain to temporal & frontal lobes of the cerebral cortex | Cognition, communication social function, response to stress | Relief of Psychosis, Akathisia? |
| Tuberoinfundibular | hypothalamus to the median eminence of the anterior pituitary | Regulates prolactin release | Increased prolactin Concentrations |
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Mon Sep 05, 2011 9:19 pm
Admin Mon Sep 05, 2011 9:19 pm
 [img][/img]
[img][/img]Freud proposed three structures of the psyche or personality:
Id: a selfish, primitive, childish, pleasure-oriented part of the personality with no ability to delay gratification.
Superego: internalized societal and parental standards of "good" and "bad", "right" and "wrong" behaviour.
Ego: the moderator between the id and superego which seeks compromises to pacify both. It can be viewed as our "sense of time and place"
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Tue Sep 06, 2011 7:23 pm
Admin Tue Sep 06, 2011 7:23 pm
C/C: fatigue
HOPI: For past 2-3 weeks, c/o profound tiredness, increased need for sleep & increased appetite. These symptoms started after a break up with her boyfriend.
Pt's symptoms rapidly improved after she reunited with her boyfriend.
What is the diagnosis:
(a) Bipolar disorder with rapid cycling
(b) Borderline personality disorder
(c) Major depression with Atypical features.
*************************************************
Answer: Major depression with Atypical features
*************************************************
Explanation:
This is an important question, because "Major depression with Atypical features" is the most common subtype of depression (so more chances of questions on this topic on PRITE & related exams).
Look for following points:
(1) Mood brightens in response to actual or potential positive events (Compared to Melancholic subtype: mood doesn't brighten even in response to positive events).
(2) 2 or more of following features:
- Significant weight gain/increase in appetite
- Hypersomnia
- Leaden paralysis (heavy, leaden feelings in arms & legs)
- Long standing pattern of interpersonal rejection sensitivity that results in significant social & occupational impairment.
Last edited by Admin on Sun Sep 30, 2012 12:00 am; edited 2 times in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() psychinmymind Tue Sep 06, 2011 9:47 pm
psychinmymind Tue Sep 06, 2011 9:47 pm
psychinmymind- Moderator
- Posts : 24
Points : 44
Reputation : 3
Join date : 2011-04-14
Location : Arizona
Re: PRITE High Yield Topic Discussion Thread
![]() psychinmymind Tue Sep 06, 2011 9:47 pm
psychinmymind Tue Sep 06, 2011 9:47 pm
late onset of presentation and responds to drug dosage decrease or antiparkinsonian agents
psychinmymind- Moderator
- Posts : 24
Points : 44
Reputation : 3
Join date : 2011-04-14
Location : Arizona
Re: PRITE High Yield Topic Discussion Thread
![]() psychinmymind Tue Sep 06, 2011 9:50 pm
psychinmymind Tue Sep 06, 2011 9:50 pm
mania than clozapine. Clozapine appears to control manic states much better than depressive states.
psychinmymind- Moderator
- Posts : 24
Points : 44
Reputation : 3
Join date : 2011-04-14
Location : Arizona
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Tue Sep 06, 2011 9:54 pm
Admin Tue Sep 06, 2011 9:54 pm
psychinmymind wrote:Risperidone appears to have higher efficacy in patients with psychosis and depression, but is more likely to cause
mania than clozapine. Clozapine appears to control manic states much better than depressive states.
Good Info PsychInMyMind. What is the source of this information (any citations). Thanks
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() psychinmymind Tue Sep 06, 2011 10:09 pm
psychinmymind Tue Sep 06, 2011 10:09 pm
psychinmymind- Moderator
- Posts : 24
Points : 44
Reputation : 3
Join date : 2011-04-14
Location : Arizona
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Tue Sep 06, 2011 10:11 pm
Admin Tue Sep 06, 2011 10:11 pm
psychinmymind wrote:taught in our didactics
Thanks for sharing. Keep up the good work

Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Thu Sep 08, 2011 12:38 pm
Admin Thu Sep 08, 2011 12:38 pm
1. Paranoid Personality Disorder
| Paranoid Personality Disorder | Delusional disorder and Schizophrenia |
| Reality testing intact | Reality testing lost |
| Paranoid Personality Disorder | Schizoid and Avoidant personality disorder |
| Amount and Degree of paranoia is significantly less |
2. Schizoid Personality Disorder
| Schizoid Personality Disorder | Schizophrenia |
| 1. Reality testing intact | Reality testing not intact |
| Abstracting ability normal | Abstracting ability impaired |
| Presence of formal thought process | formal thought process impaired |
| Schizoid Personality Disorder | Paranoid Personality Disorder |
| Less socially oriented ideations | More socially oriented ideations |
| Amount and Degree of paranoia is significantly less |
| Schizoid Personality Disorder | Obsessive Compulsive & Avoidant Personality Disorder |
| often socially isolated, but view loneliness as ego-dystonic or ego-alien and they enjoy a richer interpersonal history |
3. Schizotypal Personality Disorder
| Schizotypal Personality Disorder | Paranoid & Schizoid Personality Disorder |
| Share many core features; but differs by degree or absence of eccentricity |
| Schizotypal Personality Disorder | Borderline Personality Disorder |
| Share unusual speech & perceptual style; but demonstrates stronger affect & connection to others |
| Schizotypal Personality Disorder | Avoidant Personality Disorder |
| Also uncomfirtable & inept in social situations; but are not eccentric & crave for contact with others. |
| Schizotypal Personality Disorder | Schizophrenia |
| 1) Reality testing lost. 2) Psychosis present |

Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Thu Sep 08, 2011 5:16 pm
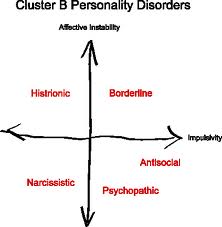
Admin Thu Sep 08, 2011 5:16 pm
- Share the common features of being dramatic, emotional, and erratic
- Said to combine abnormalities in both thinking and affect, but not to be predominantly one or the other cluster, such as cluster A (thinking) or cluster C (affect)
1. Antisocial Personality Disorder
| Antisocial Personality Disorder | Borderline Personality Disorder |
| demonstrate more repetitive suicidal and parasuicidal behaviors, as well as intense affect and self-loathing |
| Antisocial Personality Disorder | Narcissistic Personality Disorder |
| Blue collar crime (primary motivation is short-term material gain) | White collar crime (primary motivation is to maintain their grandiose self-image- power and money) |
| Antisocial Personality Disorder | Bipolar Mania |
| often lack a significant degree of childhood conduct problems, & antisocial behavior is usually limited to manic episodes |
| Antisocial Personality Disorder | Substance abuse disorder |
| criminal behaviors associated with substance abuse disorders generally center around using and obtaining the drugs |
2. Borderline Personality Disorder
| Borderline Personality Disorder | Histrionic, Narcissistic, & Dependent disorders |
| more stable identities & rarely engage in self-mutilation or chronic suicidal behaviors |
| Borderline Personality Disorder | Bipolar Spectrum Disorder |
| mood swings does not meet criteria for manic or hypomanic episodes | mood swings meet criteria for manic or hypomanic episodes |
3. Histrionic Personality Disorder
| Histrionic Personality Disorder | Narcissistic Personality Disorder |
| is more outwardly emotional and deeply involved with others | lack empathy for others ; and more preoccupied with grandiosity and envy |
| Histrionic Personality Disorder | Dependent Personality Disorder |
| Both shares the need for acceptance and reassurance; DPD lacks the degree of emotionality seen in histrionic individuals |
| Histrionic Personality Disorder | Dependent Personality Disorder |
| Both shares the need for acceptance and reassurance; DPD lacks the degree of emotionality seen in histrionic individuals |
| Histrionic Personality Disorder | Somatization disorder |
| greater emphasis on physical complaints |
4. Narcissistic Personality Disorder
| Histrionic Personality Disorder | Narcissistic Personality Disorder |
| is more outwardly emotional and deeply involved with others | lack empathy for others ; and more preoccupied with grandiosity and envy |
| Antisocial Personality Disorder | Narcissistic Personality Disorder |
| Blue collar crime (primary motivation is short-term material gain) | White collar crime (primary motivation is to maintain their grandiose self-image- power and money) |
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() psychinmymind Thu Sep 08, 2011 10:35 pm
psychinmymind Thu Sep 08, 2011 10:35 pm
Early loss of social skills----------Social skills preserved until late
Memory loss late in disease----------Memory loss often presenting symptom
Early loss of executive function----------Late loss of executive function
Stereotyped speech with terminal mutism----------Fluent aphasia
Semantic anomia----------Lexical anomia
Visuospatial deficits late in disease----------Visuospatial deficits characteristic
Frontotemporal hypoperfusion/hypometabolism----------Parietal and posterior temporal abnormalities
No specific neuron type affected----------Cholinergic neurons targeted
Initial presentation of personality change----------Personality change is late
psychinmymind- Moderator
- Posts : 24
Points : 44
Reputation : 3
Join date : 2011-04-14
Location : Arizona
Re: PRITE High Yield Topic Discussion Thread
![]() psychinmymind Thu Sep 08, 2011 10:41 pm
psychinmymind Thu Sep 08, 2011 10:41 pm
By contrast, heteroreceptors are receptor subtypes that are present on neurons that do not contain an endogenous ligand for that particular receptor subtype (e.g., a serotonergic receptor located on a dopaminergic neuron).
psychinmymind- Moderator
- Posts : 24
Points : 44
Reputation : 3
Join date : 2011-04-14
Location : Arizona
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Fri Sep 09, 2011 11:17 am
Admin Fri Sep 09, 2011 11:17 am
1. Avoidant Personality Disorder
| Avoidant Personality Disorder | Schizoid Personality Disorder |
| Desire relationships with others | Do not desire relationships with others |
| Avoidant Personality Disorder | Dependent Personality Disorder |
| greater fear of abandonment, and embraces, rather than avoids, relationships |
| Avoidant Personality Disorder | Social phobia |
| more specific fears around social performances |
2. Dependent Personality Disorder
| Dependent Personality Disorder | Histrionic Personality Disorder |
| Both shares the need for acceptance and reassurance; DPD lacks the degree of emotionality seen in histrionic individuals | have issues of dependency, but shorter and more numerous relationships |
| Dependent Personality Disorder | Borderline Personality Disorder |
| become more placating around real or perceived abandonment | express more affect and anger around real or perceived abandonment |
| Dependent Personality Disorder | Avoidant Personality Disorder |
| When faced with rejection or termination of a relationship, they quickly seek out a new relationship to fill the void | When faced with rejection or termination of a relationship, they withdraw from further contact |
| Dependent Personality Disorder | Agorophobia |
| higher level of fear around leaving specific safe environments, especially home |
3. Obsessive-Compulsive Personality Disorder
| Obsessive-Compulsive Personality Disorder (OCPD) | obsessive-compulsive disorder (OCD) |
| have true obsessions and compulsions that they find ego-dystonic | find that their behaviors are ego-syntonic and rewarded by others |

Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Fri Sep 09, 2011 12:22 pm
Admin Fri Sep 09, 2011 12:22 pm
Cluster A Personality Disorders- Differential Disgnosis. http://bit.ly/qVvufk
Cluster B Personality Disorders- Differential Disgnosis. http://bit.ly/qKFSsl
Cluster C Personality Disorders- Differential Disgnosis. http://bit.ly/qEAhR0
Facts:
- Schizotypal Personality Disorder: there appears to be a higher occurrence of this disorder in the biological relatives of schizophrenic patients, and the disorder is frequently diagnosed in women with fragile X syndrome.
- Personality disorders in cluster B are said to combine abnormalities in both thinking and affect, but not to be predominantly one or the other cluster, such as cluster A (thinking) or cluster C (affect).
- Because patients with antisocial PD are so indifferent to how their actions affect others, this is the personality disorder most resistant to treatment.
- Patients with antisocial PD have an onset of conduct disorder before age 15, and frequently suffer from co-morbid attention-deficit/hyperactivity disorders, polysubstance disorders, and somatization disorder. The exact etiology is unknown, but this disorder occurs five times more commonly in first-degree relatives of males with the disorder
- Under stress, borderline patients may also experience brief reactive psychotic states (also known as “micropsychotic episodes”)
- BPD is the most prevalent personality disorder in all clinical settings (12% to 15%)
- Some believe that while not all borderline patents are histrionic,but most HPD patients have sufficient borderline traits to merit a diagnosis of BPD.
- Narcissistic Personality disorder pt lack empathy for others, although less so than the antisocial patient
- For some narcissistic patient, aging is the ultimate blow to their self-esteem, as many of the qualities that help maintain their identity (e.g., career, health, beauty, and youth) must naturally begin to fade. Consequently, the narcissistic patient is prone to severe midlife crises.
- Avoidant PD are at especially high risk for anxiety disorders and for social phobia
- Patients with a history of childhood separation anxiety or chronic illness may be predisposed to the Dependent personality disorder.
- Interviewing for signs and symptoms of a personality disorder requires a longitudinal developmental perspective. Such longitudinal interviewing should assess the quality of the patient's social function in the areas of school, career, family, romantic relationships, peer group function, and interactions with authority figures. Across these categories, clinicians should listen for recurring themes of interpersonal conflict, disappointment, exploitation, or emptiness, because these can all indicate a personality disorder.
- While personality-disordered individuals often use lower-level defense mechanisms, such as projection and denial, and commonly disown responsibility for their actions, they often confirm a public or family consensus about their behavior if couched in sympathetic terms: “Have you ever been unjustly accused of taking things at your various jobs? How often?” “Do people fail to understand and admire your assertiveness and your refusal to get pushed around? Really? Tell me about that.”
- Patients with cluster C disorders improve more than patients with borderline personality disorder, while borderline patients improve more than schizotypal and antisocial personality-disordered patients.
- Patients with a cluster B personality disorder have a dropout rate of 40%, a cluster A disorder of 36%, and a cluster C disorder of 28%. Patients in group therapy have a higher dropout rate than do patients in individual therapy
- Select pharmacotherapy on the presence of specific target symptoms rather than on a given personality disorder diagnosis
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Fri Sep 09, 2011 1:33 pm
Admin Fri Sep 09, 2011 1:33 pm
psychinmymind wrote:Frontotemporal dementia ----------Alzheimer’s dementia
Early loss of social skills----------Social skills preserved until late
Memory loss late in disease----------Memory loss often presenting symptom
Early loss of executive function----------Late loss of executive function
Stereotyped speech with terminal mutism----------Fluent aphasia
Semantic anomia----------Lexical anomia
Visuospatial deficits late in disease----------Visuospatial deficits characteristic
Frontotemporal hypoperfusion/hypometabolism----------Parietal and posterior temporal abnormalities
No specific neuron type affected----------Cholinergic neurons targeted
Initial presentation of personality change----------Personality change is late
Semantic Anomia:
- Patients appear to suffer interference between related concepts (e.g., tiger-lion).
- Some patients can name natural kinds but not human artifacts, or vice versa.
- Utter grammatically correct speech that has no relevance to the conversation at hand ''
What is Lexical Anomia?.
Thanks
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Re: PRITE High Yield Topic Discussion Thread
![]() Admin Fri Sep 09, 2011 10:17 pm
Admin Fri Sep 09, 2011 10:17 pm

| Lesion | Defect | Causes |
| (1)- Left Optic Nerve | Left Monocular Visual Loss | Trauma, Multiple Sclerosis |
| (2)- Optic Chiasma | Bitemporal Hemianopia | Pituitary Tumors |
| (3)- Optic tract | Homonymous Hemianopia | Stroke, Space Occupying Lesions |
| (4)- Lt Temporal Optic Radiation (Meyer's Loop) | Rt Homonymous Superior Quadrantanopia | Stroke, Space Occupying Lesions |
| (5)- Lt Parietal Optic Radiations | Rt Homonymous Inferior Quadrantanopis | Stroke, Space Occupying Lesions |
| (6)- Lt Occipital Lobe | Rt Homonymous Quadrantanopia with Macular Sparing | Stroke (Posterior Circulation) |
Last edited by Admin on Sat Sep 14, 2013 6:51 pm; edited 1 time in total
Admin- Admin
- Posts : 948
Points : 2102
Reputation : 0
Join date : 2011-02-19
Location : Philadelphia -
Page 1 of 4 • 1, 2, 3, 4 ![]()
» Personality Disorders (10 High Yield Facts)
» prite question
» prite exam
» PRITE Oriented Topics
FORUM FOR PSYCHIATRY RESIDENTS :: Psychiatry :: Psychiatry-Neurology-Psychology discussion :: Psychiatry In Depth
» L-Methylfolate: Who Will benefit
» Vitamins & Supplements in Clinical Practice.
» Imaging Biomarkers for Outcomes in Mild TBI
» Q.5 Clozapine Neutopenia
» Treating Disorders!
» Cortical Abnormalities in Adults & Adolescents with MDD
» Efficacy of Antipsychotics in Pediatric Acute Mania
» Obsessive Compulsive Disorder in Adults: Which Treatment is Better?